

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Since Phillipe Mouret of France performed the first laparoscopic cholecystectomy (LC) in 1987, multiport conventional LC (CLC) has become the gold standard for the treatment of gallbladder (GB) disease [1], with advantages of better cosmesis, less scar, less pain, and shorter hospitalization [2]. Surgeons have attempted to reduce number of ports and incisions with accumulation of experience and development of equipments for the past few decades. Single incision laparoscopic cholecystectomy (SILC) was first performed by Navarra et al. [3] in 1997, but did not regain much popularity since the development. However, the recent increase in use of SILC can be attributed to new surgical techniques and equipment, such as the articulating instruments and access ports capable of allowing several instrument to be inserted in a single ports [4,5,6]. Nowadays, the 3-channel method with multiport access is commonly used in SILC [7]. Despite the new techniques and exponential improvement of equipment, there still remains some limitations, such as difficulty in exposure of the Calot's triangle, narrow indications (exclusion criteria: high body mass index [BMI], previous abdominal surgery, acute cholecystitis with severe gallbladder [GB] inflammation), and higher bile duct injury rate with the 3-channel SILC [8,9]. For these reasons, adequacy and feasibility of SILC is still controversial. Previously, we had also performed 3-channel SILC with 2 instruments and a flexible telescope, but encountered similar limitations. Therefore, we have replaced our standard setting into a 4-channel SILC with an addition of a snake retractor for resolution of the aforementioned limitations. In this study, we hereby report an adequacy and feasibility of 4-channel single incision laparoscopic cholecystectomy using a snake retractor.
METHODS
We have conducted retrospective review of 415 patients that underwent SILC between April 2010 and February 2013. From April 2010 through September 2012, 326 patients had been treated with 3-channel method using a handmade single port, a flexible telescope and two articulating instruments. In the early period, we excluded those who were older than 70 years of age with radiologic or pulmonologic comorbidities, or acute GB inflammation, but did not exclude patients with high BMI or history of abdominal surgery. After 50 cases, with accumulation of experience, the inclusion criteria of SILC was expanded to all the patients who would typically be considered for CLC, but excluded the patients with suspected early-staged GB malignancy [10]. After October 2012, we have modified our 3-channel method to a 4-channel SILC by adding a snake retractor for liver retraction which we later named as "modified Konyang standard method". Eighty-nine patients have been treated with the 4-channel SILC using a snake retractor, and the inclusion criteria for the 4-channel SILC had been applied equally.
Instruments and port
The handmade port consisted of a 10-mm size ALEXIS wound retractor (Applied Medical, Rancho Santa Margarita, CA, USA) and size 7 sterile glove in which three 5-mm ports and one 10-mm port (Laport, Sejong Medical, Paju, Korea) were prepared on the 1st, 2nd, 3rd, 5th tip of fingers to create a 4-working channel for the laparoscopic instruments (Fig. 1). The wound retractor was introduced through 2.5-cm transumbilical incision. The surgical glove was fixed to the outer ring of the wound retractor and then the CO2 pipe was connected to 10-mm port to create pneumoperitoneum. We used a 10-mm flexible telescope (Olympus Co., Tokyo, Japan), a 5-mm snake liver retractor for liver traction (Diamond-Flex Triangular Retractors, CareFusion, Waukegan, IL, USA), a long articulated Endo-Roticulator (Coviden, Mansfield, MA, USA) for traction and dissection of GB, and a suction-hook bovie (Endopath Probe Plus II Pistol Grip Handle, Ethicon Endo-Surgery Inc., Cincinnati, OH, USA) for irrigation and coagulation. We ligated cystic duct and artery using 5-, 10-mm Hem-O-Lok clip (Weck Closure Systems, a division of Teleflex Inc., Wayne, PA, USA).
Surgical technique
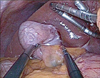
The patients were placed in reverse Trendelenburg position (15-30 degrees) with right side up. A 2.5-cm transumbilical incision was made and the handmade port was inserted. After making pneumoperitoneum, a flexible telescope was inserted through 3rd finger channel and then snake retractor was inserted through 2nd finger below the telescope. The snake retractor was angulated and retracted the liver. The GB was retracted laterally with a grasper which was inserted through 5th finger and the anterior peritoneum surrounding the cystic duct was dissected by left hand using a dissector through 1st finger channel (Fig. 2). After that, the left hand performed cephalic traction of the infundibulum and exposed the posterior peritoneum of the cystic duct, and then the grasper held in the right hand carried out posterior peritoneal dissection. Isolation of the cystic duct and artery using 30-50 degrees angulated dissector held in the left hand was performed. After isolating the cystic duct, both the duct and the artery are clipped using 5-mm Hem-O-Lok clip held in the left hand and the cystic duct and artery were divided using scissors held in the left hand. After the cystic artery and duct were divided, the GB was pulled cephalad using the grasper held in the right hand and then the GB was dissected from the GB bed using the suction-hook bovie held in left hand. After irrigation by the right hand using the suction-hook bovie, the GB was removed through the Alexis wound retractor positioned at the umbilical incision without an endo-bag.
RESULTS
Preoperative clinical characteristics
Among 415 SILC patients, there were 189 male (45.5%) and 226 female patients (54.5%). The mean age was 52.3 ± 14.0 years old, and the mean BMI was 25.7 ± 15.1 kg/m2. One hundred and nineteen patients (28.7%) had previous abdominal surgeries, and 10 of 119 patients had undergone upper gastrointestinal (GI)surgery. The mean operation time was 52.7 ± 24.4 minutes, and the mean hospital stay was 2.9 ± 3.0 days. Conversions to CLC that required additional ports were 9 cases (2.1%) (Table 1).
Comparisons between 3- and 4-channel SILC
Three hundred and twenty-six patients underwent 3-channel SILC, and 89 patients had the 4-channel SILC using a snake retractor. There were 143 male (43.9%) and 185 female patients (56.1%) in the 3-channel SILC group whereas 46 male (51.7%) and 43 female patients (48.3%) in the 4-channel SILC group. Previous operative history were present on 96 patients (29.4%) of which 7 cases had undergone upper GI operation vs. 23 cases (25.8%) with 3 cases of upper GI operation (P = 0.505). Mean BMI was 25.7 ± 17.0 kg/m2 vs. 25.2 ± 3.9 kg/m2 (P = 0.806), 30 patients (9.2%) vs. 23 patients (25.8%) were treated with percutaneous transhepatic gallbladder drainage (PTGBD) insertion before operation (P < 0.001), mean operating time was 53.0 ± 25.8 minutes vs. 51.9 ± 18.6 minutes (P = 0.709) and mean hospital stay was 3.0 ± 3.3 days vs. 2.6 ± 0.9 days (P = 0.043). There were total 9 cases (2.1%) of port addition, 6 cases (1.8%) in the 3-channel group and 3 cases (3.4%) in the 4-channel group (P = 0.411), due to cystic artery bleeding and bile leakage from the GB bed, but there were no open conversions. There was no statistically significant difference between the 3-channel SILC and the 4-channel SILC group except for PTGBD insertion (P < 0.001) and mean hospital stay (Table 2).
Postoperative complications between 3- and 4-channel SILC
Postoperative complications were observed in total of 7 patients, 6 cases in the 3-channel group and 1 case in the 4-channel group (Table 3). Of the 7 patients, 2 were major complications requiring additional treatments (1 bile duct injury and 1 duodenal perforation), and the remaining 5 were minor complications (4 wound infections and 1 incisional hernia). In the 4-channel SILC group, 1 wound infection was observed. There was no mortality. Bile duct injury occurred in a patient with severe GB inflammation, was determined to be type E by Strasberg's classification, detected at postoperative day 2, and was treated with hepaticojejunostomy. For the patient with duodenal perforation, there was severe adhesion between the duodenum and the liver from prior subtotal gastrectomy. The duodenal perforation had most likely occurred during dissection of the duodenum that was firmly adhered to the liver. Signs and symptoms of peritonitis were observed at postoperative day 2, and it was treated with laparoscopic primary repair of perforation site. The four patients with wound infections were treated with simple dressing. Incisional hernia occurred in a patient who was treated for wound infection after postoperative month 3, and herniorrhaphy was performed. All complications occurred in the 3-channel SILC group except for 1 simple wound infection.
DISCUSSION
Since Phillipe Mouret of France performed the first LC in 1987 [1], the superiority of LC as the standard procedure for GB removal compared to the open cholecystectomy has not been questioned due to better cosmetic satisfaction, less scar, less pain, and shorter hospitalization [2]. Ever since the initial development of LC, surgeons had attempted to reduce the number and the size of ports. In these efforts, more challenging and innovative methods like natural orifice transluminal endoscopic surgery (NOTES) have been invented and developed. Since the first NOTES transvaginal cholecystectomy by Bessler et al. [11] of the United States in 2007, numerous NOTES cholecystectomies have been performed. However, some challenges still exist, including longer operating time, poor triangulation of instruments, difficulty in standardization of the procedure, and increased risks of leakage and fistula, which clearly indicates that improvement of the NOTES surgical techniques and instruments is much needed [7,11]. Nowadays, surgeons have switched their focus to single incision laparoscopic surgery as an alternative minimally invasive surgery to the NOTES. Since the first SILC by Navarra et al. [3] in 1997, various new techniques and instruments have been introduced and modified. SILC has become more popular, and several studies including review of over hundred cases or meta-analysis of the operative data have been reported [12,13,14,15,16]. The SILC certainly has superior cosmetic outcome compared to the CLC. However, a surgeon should not choose SILC solely based on superior cosmesis, patient' safety still remains as a major concern. Joseph et al. [8] reported that the bile duct injury rate in SILC (0.72%) was higher than CLC (0.2%). Trastulli et al. [16] reported a meta-analysis data including 13 randomized controlled trial studies comparing SILC vs. CLC, the failure rate was 8.4% vs. 0.7%, conversion rate to open was 0.2% vs. 0.2%, overall complication rate was 7.3% vs. 6.6% and a bile leakage rate was 0.4% vs. 0.7%. Sajid et al. [13] reported postoperative pain and complications, the hospital length of stay, cosmesis score, conversion rate, and ports addition rate were statistically similar between SILC and CLC in their meta-analysis study. Although there were various studies on SILC, the inconsistencies of results among studies ranged too wide to be certain of the safety in SILC. As we mentioned earlier, a major problem when comparing CLC and SILC is the difficulty in exposure of the Calot's triangle. Aprea et al. [17], Cao et al. [18], Edwards et al. [19], etc., many surgeons have used percutaneous anchorage with sutures and Lirici et al. [20] used needlescopic grasper for GB retraction and reducing complications. The most difficult problems of the 3-channel SILC in our department were similar to those reported from other institutes, which were inadequate visualization of the Calot's triangle and clash between the instruments and the telescope. In order to resolve these issues, we used a flexible telescope and articulating long instruments, and standardized our method, which was to retract the GB inferolaterally by right hand and to dissect the cystic duct and artery by left hand while positioning the flexible telescope at the left side of the working instruments [21]. Despite the standardization of our method, visualization of the Calot's triangle was still incomplete, especially when the GB was acutely inflamed. Thus, we incorporated a snake tractor to address the remaining issue. We had initially proposed that our modified 4-channel SILC wound have certain benefits, such as for better exposure of the Calot's triangle, and decrease in ports addition, conversion rate, and complication rate. We performed SILC in a selected patient population without severe comorbidities, or acute cholecystitis in the early period in the formerly published studies [8,22,23], but we expanded indications for SILC while increasing the number of the SILC cases, and performed 3- and 4-channel SILC on patients with major comorbidities, obesity, previous abdominal surgery, and acute cholecystitis pretreated with PTGBD, but excluded patients with possible early stage GB malignancy. A proportion of patients with acute cholecystitis, who treated with PTGBD before an operation, was 30 (9.2%) in 3-channel SILC and 23 (25.8%) in 4-channel SILC. This raises a possibility that the 4-channel SILC could be applicable for more patients with acute cholecystitis. There were total 9 cases of CLC conversion including 6 cases in the 3-channel SILC group and 3 cases in the 4-channel SILC group, due to the cystic artery bleeding. We recommended reducing this problem by ligating the cystic artery before the cystic duct ligation. There was only single wound infection case in the 4-channel SILC group and no major complication like the bile duct injury. However, there were some limitations in our study. One is the small sample size, and the other is a lower conversion and complication rate compared to other studies [13]. The latter is most likely due to the amount of experience by the surgeon who performed the 4-channel SILC, since he had previously performed over 2,000 cases of the CLC. Surely, we need larger sized samples and long-term follow-up studies. But we considered that the 4-channel SILC can become one of the primary treatments of benign GB disease in the future.
In conclusion, 4-channel single incision laparoscopic cholecystectomy has certain advantages such as better visibility and accessibility for dissection of the Calot's triangle, and reproducible methods in experienced hands. 4-channel SILC is deemed safe and feasible; therefore, most benign diseases of GB could be treated with the 4-channel SILC using a snake retractor.




 XML Download
XML Download