

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Congenital accessory limb is a very rare anomaly. The known causative factors include perinatal injury, drugs, and exposure to poisonous materials. Congenital accessory limbs are often accompanied by spina bifida and other anomalies [1,2]. Many theories have been proposed regarding the mechanism by which congenital accessory limbs develop; these include defects in the early genesis of the limb, problems arising due to a parasitic twin, or presence of a teratoma [3]. In the present report, we describe a case of a neonate born with a congenital accessory limb and imperforate anus that was not detected by prenatal sonography during the gestational period.
CASE REPORT
The female patient was born via vaginal delivery after a 38-week gestational period. At birth, the patient's weight was 3.0 kg and her height was 52 cm. The patient had a cephalic, abdominal, and thoracic circumference of 33 cm, 30 cm, and 32 cm, respectively. Her mother was 27 years old at the time of the patient's birth. Neither parent had a remarkable medical, family, or gynecologic history. The mother's pregnancy was uneventful, and no complications developed, except for oligohydramnios. However, after birth, the patient was found to have a congenital accessory limb on a buttock with 4 toes (Fig. 1), and was therefore transferred from the local medical center to our facility.
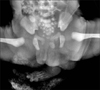
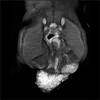
Below the accessory limb, we found a small anal opening on the perineal body, which involved the anterior portion of the external sphincter. However, the urethral and vaginal openings were normal. The patient was diagnosed with imperforate anus with perineal fistula. She had no urogenital anomalies and cardiac anomalies, and small patent ductus arteriosus was noted. An infantogram indicated the presence of oval-shaped bony structures below the sacrum (Fig. 2). To evaluate the pelvic organs, associated anomalies, and the anatomy of accessory limb, we performed MRI. Moreover, no spinal anomaly was present, but an ossified oval-shaped bone, an ossified long bone, and a nonossified long bone around the limb were observed (Fig. 3). As these abnormal bones occupied the pelvic region, the rectum was deviated to the right side. Although the patient could still pass stools to some extent, a major portion of the anus was closed. We initially performed a cut-back anoplasty and excised the accessory limb. Two long bones, similar to the tibia and fibula, were found to connect the accessory limb to the buttock. Above these bones, another accessory bone, shaped like a femoral head, was located around the sacrum. All 3 bones were also excised along with the accessory limb.
Upon examination of the gross anatomy of the excised structure, the accessory limb had the appearance of a well-formed foot. However, only 4 toes were observed. These toes included nails and were curved toward the sole of the foot (Fig. 4A, B). Several under-developed bones were observed when the accessory limb was dissected, including bones that had the appearance of phalanges, metatarsals, cuneiforms bone, talus bone, and malleolus bone (Fig. 4C). On microscopic observation, these bones were found to comprise undeveloped bony structures and cartilage, and included bone marrow (Fig. 5A). In addition, the bones were surrounded by body fat, muscles, and blood vessels (Fig. 5B). However, neuroglial cells and excess tissues, such as harmatoma, were not observed under the microscope. The patient's recovery course was uneventful, but the shape of buttock remained asymmetric (Fig. 6). During the follow-up period of 8 months, she was found to be in a good condition, and could defecate well without constipation.
DISCUSSION
The first report of an accessory limb was published in 1975, and involved a baby born with 3 limbs [4]. Other cases of congenital accessory limb were subsequently reported, and many of these cases were accompanied by spina bifida or other neurologic deformities [2,5]. Many studies also provided suggestions of possible causes of accessory limb formation, such as problems with limb bud generation, problems related to a parasitic twin, or the presence of a teratoma.
Due to the presence of multiple limbs, congenital accessory limb can be diagnosed as a remnant of a parasitic twin. However, this diagnosis can be easily excluded in the present case, because cases of parasitic twin are usually accompanied by urologic deformities or anorectal deformities as a consequence of the twin [6].
In contrast, there have been cases where teratomas have been diagnosed as accessory limbs. A recent report by Unterscheider et al. [7] is one such case, where a structure initially diagnosed as an accessory limb with syndactyly was found to be a teratoma upon microscopic examination. Moreover, Sharma et al. [2] reported 3 cases with accessory limb, and confirmed that the well-developed limb was not a teratoma. In the present case, we performed histologic examination on the excised accessory limb, but could not obtain any evidence indicating that this structure was a teratoma.
During fetal development, a limb bud is composed of mesenchymal tissue, which originates from the mesoderm and surrounding ectodermal tissue. Previous case reports have suggested that, because the spine also originates from the mesoderm, spinal deformities-such as spina bifida-can be accompanied with an accessory limb if a problem arises in the mesoderm during the early phase of limb bud development [2,8]. Verma et al. [9] reported the case of a club-footed accessory limb attached to the acetabulum. These deformities do not typically accompany each other, and therefore, it was suggested that the deformity was a result of problems in limb bud development.
In the present case, although spinal deformities were not noted, an anorectal malformation was observed. The accessory limb was attached on the left side of the sacrum. As the anus originates from the ectoderm-like neurologic system and limb bud originates from the mesoderm, we believe that there is no relationship between the accessory limb and the anal deformity observed. We hypothesize that simultaneous defects in the mesoderm and ectoderm may have resulted in the development of an accessory limb along with an imperforate anus, or the accessory limb may have pushed the anus during development finally resulting in a low type of imperforate anus.
Unterscheider et al. [7] reported 3 cases of accessory limbs diagnosed after birth and demonstrated the effectiveness of MRI in the diagnosis of congenital accessory limb. Although it is believed that congenital accessory limbs are easy to diagnose prenatally because of its apparent appearance, it was difficult to diagnose this condition prenatally in the present patient. One of the reasons for the difficulty in the detection of this condition in general is that pelvic examination is not usually performed during sonographic evaluation in local clinics. Furthermore, radiologic evaluation failed to detect the bony tissue in the buttock. As such cases of nonossified deformities can also occur, we believe that multimodal imaging studies should be performed prior to the surgical excision of congenital accessory limbs.




 XML Download
XML Download