

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Inguinal hernia repair is one of the most common operations around the world [1]. Laparoscopic total extraperitoneal (TEP) repair of inguinal hernia had been proposed early in 1990, and the proportion of laparoscopic hernia surgery has consistently increased [2,3]. Laparoscopic TEP has several benefits including less postoperative pain, early ambulation, and lower recurrence rate [4,5]. However, there are some obstacles that keep laparoscopic TEP from spreading rapidly; these are related to steep learning curve, narrow operative field, and unfamiliar anatomic structure to surgeons [6].
In particular, laparoscopic TEP sometimes gets demanding during surgery, in case of bleeding, unusual anatomic structures, hard extraperitoneal dissection, and especially peritoneal tearing. Surgeons on a learning curve are weak in dealing with these situations. Thus, these technically demanding aspects can cause prolonged operative time, conversion to open procedure, and complications [7,8]. If laparoscopic TEP converts to open procedure, patient's satisfaction decreases owing to higher cost, additional surgical wound, prolonged operative time, and more postoperative pain [9]. If, during learning curve, surgeons select technically nondifficult inguinal hernia cases before operation, it may help them overcome the learning curve of laparoscopic TEP more easily. However, few studies on this topic have been found in the literature.
The present study was conducted to identify clinical factors that can influence technical difficulty with laparoscopic TEP according to learning period.
METHODS
Patient selection
We conducted a retrospective study of 112 adult patients who underwent unilateral inguinal hernia repair from January 2009 to September 2013. Patients below the age of 17, with femoral hernia or ventral hernia, bilateral inguinal hernia, cooperation with other surgery, and urgent hernia surgery due to peritoneal sign or incarceration were excluded from the study. All operations were performed by two surgeons. TEP procedure was utilized in all laparoscopic hernia repairs.
Laparoscopic TEP repair
An oblique 2-cm incision is made below the umbilicus. Then a small incision is made in the anterior sheath of the rectus abdominis muscle. A track along the posterior sheath is created with a retractor. The preperitoneal space is dissected to symphysis pubis with balloon dissector system (Autosuture, Mansfield, MA, USA). If some obstacles are expected such as adhesion due to previous abdominal surgery or bleeding tendency, direct telescopic dissection is performed with laparoscopic camera. After the establishment of preperitoneal space, the balloon is removed and the space is insufflated with CO2 to a pressure of 12 mmHg.
Another 5-mm trocar is placed 2-cm proximal to symphysis pubis, and the other 5-mm trocar is placed in the middle of the two trocars. Dissection is extended laterally with identification of the inferior epigastric vessels. Peritonealization of the hernia sac and parietalization of the vas deference and spermatic vessels are carried out. Parietex mesh (Autosuture) is applied in the inguinal lesion to reinforce the abdominal wall. The mesh is placed covering the whole myopectineal orifice and is fixed to the anterior abdominal wall with 5-mm protack (Autosuture).
Clinical variables
Clinical characteristics were compared between learning period and experience period of laparoscopic TEP. Several clinical factors were analyzed to identify impact on technical difficulty with hernia repair according to learning period. Technical difficulty was defined by operative time, major complication, or open conversion. Operative time was categorized at the 70th percentiles of the distribution curve in each surgeon as difficult group (≥70th percentile) and nondifficult group (<70th percentile). Previous abdominal surgery cases were confined to incise peritoneum level on the same side. Previous hernia surgery cases were restricted to ipsilateral side. Major complications were comprised of visceral injury, vascular injury, symptomatic hematoma, and vas deference or testicular vessels injury. Minor complications consisted of seroma, mild hematoma, scrotal swelling, and urinary retention. BMI was categorized according to 25 kg/m2, which is regarded as Asian obesity index in World Health Organization guidelines [10]. Learning period was split by the 30th case of each operator, which was considered to be the learning curve in a previous study [11]. All clinical information was based on the daily described medical records.
Statistical analysis
The independent-samples T test was utilized to compare means of normally distributed continuous variables. The Mann-Whitney U-test was used to compare means of not normally distributed continuous variables. Chi-square test or Fisher exact test was applied to compare the frequencies of categorical variables. Multivariate analysis was performed with logistic regression analysis using a backward likelihood ratio approach. The cutoff P-value was set at 0.1 and the statically significant entry and staying values were set at 0.005. P-value less than 0.05 was considered statistically significant. For the analyses, IBM SPSS Statistics ver. 21.0 (SPSS Inc., Chicago, IL, USA) statistical analysis software was used.
RESULTS
Patient characteristics
There was no difference between learning period and experience period except operative time and postoperative hospital stay (Table 1). Surgeon 1 has performed the same number of laparoscopic TEP as surgeon 2. Operative time has decreased by 30% for surgeon 1 and 10% for surgeon 2 between the two periods. Perioperative major and minor complications were similar between the two periods.
Comparison between technical difficulty and perioperative clinical factors
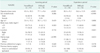
The rate of BMI above 25 kg/m2 was significantly higher in the difficult group than the nondifficult group during the learning period of laparoscopic TEP (P = 0.020) (Table 2). On the other hand, it revealed no statistical difference with technical difficulty during the experience period (P = 0.882). Previous hernia surgery was not significantly related to the difficult group in both learning period and experience period of laparoscopic TEP. Hernia type and location did not influence technical difficulty with laparoscopic TEP.
Multivariate analysis
BMI (≥25 kg/m2) was identified as a significant independent factor for technical difficulty with laparoscopic TEP in the learning period (P = 0.015) (Table 3).
DISCUSSION
Inguinal hernia has been managed with various surgical methods. However, it is controversial as to which surgical technique is superior to others [12,13]. Recently, laparoscopic repair of inguinal hernia has been applied more frequently than in the past owing to the development of laparoscopic devices and surgical techniques [3]. The purpose of this study was to identify clinical factors for technical difficulty with laparoscopic TEP according to learning period.
Technically challenging situations during laparoscopic hernia repair are caused by various factors, e.g., uncontrolled bleeding, demanding extraperitoneal dissection, and peritoneal tearing [9]. In these cases, operative time would generally increase and laparoscopic approach could be converted to open procedure. Additionally, perioperative major complications could occur. Therefore, extension of operative time, conversion to open procedure or occurrence of major complications can be interpreted as technical difficulty. Accordingly, technically difficult group was defined as the cases which ranked in the 70th percentiles or more in the distribution curve of operative time, or underwent open conversion or major complication. In this study, the two surgeons performed hernia operations, and mean operative time differed between them. To correct the bias towards surgeon factor, we classified technical difficulty using percentiles in the distribution curve of operative time of the each operator, not particular time.
It is noteworthy that BMI above 25 kg/m2 was significantly relevant to technical trouble with laparoscopic TEP only in the learning period in our study. On the other hand, BMI did not correlate to technical challenge during the experience period. In the multivariate analysis, BMI above 25 kg/m2 was identified as an independent factor of technical difficulty with laparoscopic TEP (odds ratio, 4.572). The results show that the higher BMI is, the more demanding laparoscopic TEP is during the learning curve, whereas after the learning curve it is not.
This is partially consistent with the results of Schouten et al. [14], who reported that operative time was related to BMI and hernia type during laparoscopic TEP. Unlike the previous study, we evaluated the influence of BMI on the difficulty divided by the learning period. As a result, this study could demonstrate that BMI was a significant factor for the technical difficulty only in the learning period, not experience period. In addition, there were several studies that documented whether BMI was related to technical troubles with other operations besides laparoscopic TEP. Akagi et al. [15] have shown relationships between BMI and technical difficulty during laparoscopic anterior resection. Iwashita et al. [16] also reported similar results during single port laparoscopic cholecystectomy. On the other hand, Akiyoshi et al. [17] documented that BMI was not relevant to technical predicament in case of laparoscopic left hemicolectomy.
Technical difficulty related to BMI could be one of the reasons why some surgeons on a learning curve cannot overcome the high barrier to entry into laparoscopic TEP. They have sometimes abandoned the approach. The issue could prevent laparoscopic TEP from spreading rapidly. According to the study, surgeons can overcome the learning period more easily if they select inguinal hernia patients with low BMI. Afterwards, arriving at experience period, they could deal with difficulties proficiently.
We can assume three factors causing technical difficulty in high BMI patients to be as follows; first, capillary bleeding may be one of the causes. In obese patients, adipose-derived stem/progenitor cells can release multiple angiogenesis-related growth factors like vascular endothelial growth factor and hepatocyte growth factor, which can enhance angiogenesis and expand capillary network [18,19]. It might be the reason why the authors have experienced blood stained operative fields after blunt dissection with balloon dissector system during laparoscopic TEP more frequently in obese patients. Second, the obesity might affect the severity of inguinal hernia. Interestingly, several reports documented that the incidence of inguinal hernia was lower in obese people than in slim ones, although intra-abdominal pressure could be proportional to obesity [20]. The results were probably induced by delayed diagnosis due to surrounding fat tissue as well as a protective effect of the abdominal wall [21]. Delayed diagnosis can develop prolonged irritation of inguinal hernia sac and adhesion with surrounding structures. Third, a relatively narrow operative field in obese patient is technically challengeable. Obese people tend to have abundant intra-abdominal fat content especially in omentum and mesentery [19]. Therefore, a basically narrow laparoscopic operative field could be restricted more heavily by the elevated abdominal pressure in high BMI patients.
The primary limitation of this study is that two surgeons performed the inguinal hernia repair. However, both of them had carried out inguinal hernia repair in the same way. There was no difference except the average operative time. We attempted to avoid this surgeon bias by categorizing patients based on the distribution of each surgeon's operative time, not with particular time. Another limitation is in definition of technical difficulty. There could be other clinical factors besides operative time, complications and open conversion to represent technical difficulty. Prolonged operative time, conversion to open procedure, complications, and blood transfusion count were usually used as objective clinical factors to reflect learning curve and technical problems with laparoscopic surgery. Seki et al. [22] also used operative time to evaluate technical trouble with laparoscopic colectomy. Both Choi et al. [23] and Lim et al. [11] applied operative time, length of hospital stay, conversion, and complication rate to evaluate learning curve of laparoscopic TEP. In the present study, operative time, major complications and open conversion were adopted for the evaluation of technical difficulty. The tertiary limitation was that we did not inquire into other factors such as duration of hernia and distance between umbilicus and symphysis pubis which could influence difficulty with laparoscopic TEP. It is suspected that the duration of inguinal hernia may impact on the severity as previously mentioned. Also, the distance between umbilicus and symphysis pubis can affect the range of laparoscopic field. Thus, further studies are needed in this field.
In conclusion, the current study demonstrates that patient's BMI above 25 kg/m2 could create technical difficulty with laparoscopic TEP only in the learning period, not in the experience period. Therefore, BMI could be applied as one of the guidelines for inguinal hernia patient selection, especially for surgeons on a learning curve of laparoscopic TEP. It could help lower the barrier to entry into laparoscopic TEP, and further studies are needed when it comes to this topic.


 XML Download
XML Download