

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Endovascular aneurysm repair (EVAR) is minimally invasive, durable and effective for the treatment of an aortic aneurysm compared to conventional operative repair [1,2]. For successful EVAR treatment, an adequate sealing zone is necessary for stable fixation. When visceral artery branches do not have adequate proximal sealing zones, especially in cases of juxtarenal aneurysms, operators can face more complicated situations. Having an appropriate sealing zone can lead to visceral ischemia crossing vital arteries. Conversely, downsizing the sealing zone can lead to failure of fixation [3].
To solve this problem i.e., while having an adequate sealing zone in a stable segment of the aorta and preserving perfusion to the visceral branch, fenestrated and branched stent grafts have evolved.
However, these splendid inventions are high-priced and time-consuming to manufacture, so that they are not routinely available [4,5]. The chimney technique has evolved as an alternative treatment for patients with challenging anatomy and in emergency settings. The chimney technique is a placement of an auxiliary stent into the visceral artery parallel to the aortic graft.
Here, we report on a case of successful positioning of the chimney graft for preservation of a renal artery while treating a juxtarenal type I endoleak followed by a previous conventional stent graft insertion to an abdominal aortic aneurysm (AAA). During the follow up period, the chimney graft has remained patent and the type I endoleak disappeared.
CASE REPORT
A 78-year-old woman with a history of diastolic congestive heart failure and hypertension presented with an infrarenal AAA of 7.6 cm in diameter. On a computed tomogram angiography (CTA), the AAA had an infrarenal neck of 18 mm which was not too short but had severe angulation of around 85 degrees. In spite of the severe angulation, the proximal neck was sufficient and considering her old age and poor cardiac function, EVAR was a more appropriate option than open surgery.
We explained the pros and cons of the two options of EVAR and open surgery to the patient and her family; they chose EVAR rather than the open surgery.
A digital subtraction aortogram (DSA) showed an infrarenal AAA with severe neck angulation (Fig. 1). A 25-mm- × 160-mm-sized main body stent graft (Endurant Stent Graft System, Medtronic Inc., Minneapolis, MN, USA) was placed just below the left renal artery through the right femoral artery and a 24-mm- × 120-mm-sized stent graft was deployed as a contralateral limb through the left femoral artery. Ballooning was then performed using a Reliant balloon (Medtronic Inc.). Following the angiogram showed a significant amount of type I endoleak on the right side of the main body (Fig. 2). Ballooning was repeated several times and on a follow-up angiogram, the amount of leakage had decreased. Because a large amount of contrast media was used so far, we decided to stop the procedure and follow up. Her family also agreed because of her poor general condition.
On follow-up CTA after three days, it still showed a type I endoleak. Because the patient and her family wanted to leave the hospital, after seven days of close observation in the ward, she was discharged from the hospital.
After 28 days from the EVAR, she complained of abdominal pain and was admitted for evaluation of the abdomen. A CTA showed a type I endoleak and an increase in the size of the AAA to 7.9 cm. More proximal sealing was required in order to stop the endoleak. Because spare distance between the left renal artery and the main stent graft was too short to uphill the stent graft, or to place another extension stent graft, we decided on the chimney graft technique in order to obtain both an adequate sealing zone and perfusion to the renal artery.
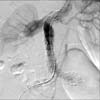
Thirty days after EVAR, a revision was performed using a chimney graft. Under general anesthesia, both common femoral arteries were punctured. Through the right common femoral artery, a pig tail catheter was placed above the aortic stent graft. An aortogram showed a large amount of type I endoleak on the right side proximal to the attachment site of the main stent graft (Fig. 3). After cutting down the left axillary artery, a 9 French sheath was inserted. The left renal artery was selected using a Cobra catheter (Cook, Bloomington, MN, USA). Rosen wire (Cook) was inserted to the distal portion of the left renal artery followed by advancement of an 8 French guiding catheter on the proximal portion of the left renal artery. A 6-mm × 50-mm Viabahn stent graft (W.L. Gore and associates, Flagstaff, AZ, USA) was then placed parallel to the aortic stent graft, covering the proximal portion of the left renal artery (Fig. 4). A 28-mm- × 52-mm-sized aortic extension (Medtronic Inc.) was inserted just below the right renal artery via the left common femoral artery. The following angiogram showed good perfusion of the left kidney and a decreased amount of type I endoleak. For the remaining, small amount of type I endoleak, ballooning was repeated. The amount of type I endoleak showed a marked decrease (Fig. 5).
On a follow-up CTA after three months, no more type I endoleak was observed, with good perfusion to the left kidney and a decrease in size of AAA to 7.7 cm. She has followed up well in the outpatient department without occurrence of any complication for 10 months of the follow-up period.
DISCUSSION
Over the past decade, EVAR has evolved as the treatment of choice for AAA. This is a reasonable choice especially for patients with high operation risks [6,7]. For anatomically challenging cases, such as short neck or severe angulation, EVAR has yielded inferior results despite short-term favorable ones [8]. Open repair remains the gold standard of treatment for AAA with a hostile aortic neck. However, as in our case, open repair showed an association with considerable mortality and morbidity in high-risk patients.
In the case of juxtarenal AAAs, fenestrated and branched technology has shown favorable results [9,10]. Despite promising results, these inventions are costly and time-consuming for tailoring to each patient which makes their routine use impossible. These endografts are not available in our country. Conversely, the chimney technique adapts daily used off-the-shelf devices in a more practical manner. Greenberg introduced the chimney technique as an adjunctive procedure involving branch vessel stenting during intentional endograft coverage of the vessel origin for maintenance of branch perfusion [4,5].
Since then, a number of studies have reported excellent early and midterm results from use of the chimney technique [7,9]. Buren et al. [7] compared early outcomes of endovascular repair of juxtarenal and suprarenal aneurysms using the chimney technique with open repair. This study concluded that the chimney technique has similar in-hospital mortality and less morbidity than open repair and cautioned that long-term durability and stent patency remain to be determined [7]. Through their experience with 21 cases, they suggested that this technique can be used in patients with high-risk and symptomatic or ruptured AAA [7]. In addition, Hiramoto et al. [9] reported a series of eight cases of single renal artery chimney stent EVAR. In this study, two patients showed a type I endoleak on immediate follow up angiography or CT scan, which was eventually resolved within one month with patency during the follow up period [9]. Use of this technique led to improved, excellent short- and medium-term results [9].
In our case, the AAA did not have a too short proximal neck, which allowed us to make a decision of conventional stent graft use. However, type I endoleak had developed at the proximal attachment site, near the renal artery. For the achievement of two critical goals (stopping the leakage while preserving renal flows), we placed the chimney graft parallel to the main aortic stent graft.
We experienced a small amount of type I endoleak during the chimney EVAR, which was resolved by three-month follow up imaging. With the chimney graft technique, a type I endoleak is usually of slow flow because the gutters between the main aortic graft, the chimney graft, and the aortic wall were created to be as narrow as possible during the procedure. Thus, a small amount of type I endoleak may have spontaneously resolved. Bruen et al. [7] mentioned that the mechanism of a seal around the chimney stents is likely multifactorial and speculated that the chimney stent induces the endograft and aortic wall to deform and seal the landing zone. However, localized rigidity of the aortic wall, as that which might occur in transmural calcifications, might be a risk factor for an endoleak after EVAR. In our case, rigidity or calcification of the aortic wall was not observed, which probably resulted in improvements of endoleak at follow-up.
In conclusion, we report a successful chimney EVAR in a patient with a juxtarenal AAA and type I endoleak. So far, early results from use of the chimney technique have been satisfactory and promising. However, long-term data and further improvement of the technique are required in order to adopt the method for widespread use.




 XML Download
XML Download