

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
HBV infection is more prevalent among patients in dialysis and in renal transplant recipients than in the general population. In Korea, the positivity rate for HBsAg among people aged 10 years or older was 3.7% of the total population being infected with HBV [1].
Pre-existing HBV infection is considered a relative contraindication to kidney transplantation. The use of immunosuppressive drugs enhances viral replication and may reactivate HBV; and this may accelerate liver injury and progression to liver failure [2]. HBV reactivation is a major risk factor for morbidity and mortality in HBsAg-positive renal transplant recipients. Moreover, HBV-associated glomerulonephritis may recur or develop de novo in the graft, reducing function and possibly resulting in graft failure [3].
Past studies established that HBsAg-positive kidney recipients are at increased risk for mortality and graft failure compared with HBsAg-negative recipients [4,5]. In the last decade, however, introduction of effective oral antiviral therapies for HBV and judicious use of immunosuppressive drugs in recipients with viral hepatitis have altered management of HBV-infected recipients [6].
In this study, we aimed to identify the outcomes of HBsAg-positive recipients who received preemptive antiviral agents after successful kidney transplantation and to analyze the risk factors for HBV reactivation.
METHODS
Patients
Lamivudine has been used at Samsung Medical Center to treat HBsAg-positive renal transplant recipients since 1999. Data for 944 patients who underwent kidney transplantation between September 1999 and September 2010 were retrieved from the electronic medical recording system and reviewed. Forty-two patients (4.4%) were categorized as HBV-infected when seropositivity for hepatitis B surface antigen was recorded on the transplant registration form. Children (<18 years old), retransplantation patients, foreigner, recipients of multiorgan transplants, and those with pretransplantation HCV infection were excluded. Data were collected for gender, age, cause of end-stage renal disease, type and duration of dialysis, HBV DNA titer before transplantation, type of transplantation, human leukocyte antigen (HLA) mismatches, induction immunosuppression and types of calcineurin inhibitor and antiviral agents used. HBV DNA was quantified using the COBAS TaqMan HBV test (detection limit 12 IU/mL, Roche Molecular Systems, Branchburg, NJ, USA). HBV DNA titers in sera were measured using a real-time PCR assay. Recipients who had taken antiviral agents before the transplantation continued with these medicines after the operation without change. Those for whom antiviral agents were not prescribed before the transplantation began lamivudine (100 mg/day) preemptively after the surgery.
All rejection episodes were confirmed by percutaneous renal biopsy. Delayed graft function (DGF) was defined by the need for hemodialysis in the first week posttransplant. Bacterial infections were diagnosed by culture results. Viral infections were diagnosed by culture results, rapid antigen detection tests, changes in serology, PCR, and cerebral spinal fluid abnormalities. Graft loss was defined as a return to dialysis, a graft nephrectomy, or retransplantation.
HBV reactivation was defined as a serum ALT concentration two times greater than the upper limit of normal, accompanied by a new detection of HBV DNA without any other cause of hepatic dysfunction. Detection of the YMDD mutation was defined as lamivudine resistance, and adefovir 10 mg/day was then added to lamivudine or patients were switched to entecavir 0.5 mg/day after consultation with a hepatologist. Survival and clinical data recorded at the time of patient death, kidney transplantation and last clinic visit up to July 2011 were assessed. This study complies with the standards of Declaration of Helsinki and current ethical guidelines.
Immunosuppression
All recipients received quadruple therapy: induction agents (ATGAM or Thymoglobulin), steroids (methylprednisolone), mycophenolate mofetil, and cyclosporine or tacrolimus. ATGAM was given at 15 mg/kg per dose for 5-7 doses, and Thymoglobulin was given at 1.5 mg/kg per dose for 5-7 doses. All doses of ATGAM and thymoglobulin were given postoperatively. Steroids were started at 500 mg per day intravenously, then tapered to 16 mg per day at 1 month posttransplantation, then to 8 mg per day at 3 months. Mycophenolate mofetil was started 1.5 g per day orally on the day of the transplantation. Cyclosporin or tacrolimus was started on posttransplant day 3.
Anti-infectious prophylaxis
Trimethoprim-sulfamethoxazole was administered for primary prophylaxis of Pneumocystis jiroveci pneumonia for at least 1 year after kidney transplantation. Other prophylactic antibiotics and antifungal drugs were not routinely administered because of the concern about emergence of resistant pathogens. All recipients received intravenous ganciclovir for 7 days. The dose of intravenous ganciclovir depended on the status of renal function in patients. They were monitored monthly for cytomegalovirus (CMV) infection by CMV antigenemia assay. If the CMV antigenemia assay showed more than 50/400,000 leukocytes, recipients were preemptively treated with intravenous ganciclovir until the CMV antigenemia assay became negative.
Statistical analysis
All statistical analyses were performed with IBM SPSS ver. 19.0 (IBM Co., Armonk, NY, USA). Continuous variables were reported as median and range or mean ± standard deviation. Cutoff value in HBV DNA was calculated by receiver operating characteristics (ROC) curve. Continuous variables were compared using Mann-Whitney U tests and categorical variables were compared using Fisher exact test. HBV reactivation-free survival was analyzed using the Kaplan-Meier method and backward in Cox regression analysis was used to determine factors related to the development of HBV reactivation. A P-value less than 0.05 was considered statistically significant.
RESULTS
Clinical characteristics for HBsAg-positive recipients
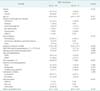
The clinical characteristics of kidney transplant recipients were summarized Table 1. Forty-two patients, including 28 men and 14 women, with a median age of 43 years (23-60 years), fulfilled the inclusion criteria. Median follow-up duration for these 42 recipients was 52.5 months (8-136 months). The underlying kidney disease was chronic glomerulonephritis in 9 patients (21.4%), diabetes in 7 patients (16.7%), hypertension in 5 patients (11.9%), IgA nephropathy in 4 patients (9.5%), unknown in 15 patients (35.7%), and others in 2 patients (4.8%). Most patients (n = 29, 69%) received hemodialysis over a median time span of 11 months (1-188 months). The mean HBV-DNA level in these patients prior to transplantation was 1.58 × 107 IU/mL. Twenty-one patients (50%) received kidney allografts from a living donor and the other patients, from deceased donors. However, the proportion of living donor kidney transplantation (LDKT) in HBsAg-negative recipients was higher than in HBsAg-positive (P = 0.001).
Graft function and graft survival
The incidence of DGF in HBsAg-positive recipients was higher than in HBsAg-negative recipients, but there was no statistically significant difference between the two groups (4.8% in HBsAg-positive vs. 1.9% in HBsAg-negative, P = 0.205). The serum creatinine in HBsAg-positive recipients was higher than in HBsAg-negative at 2 weeks (P = 0.010) because the proportion of deceased donor kidney transplantation was higher than that in LDKT in HBsAg-positive recipients. We found no significant difference in the median serum creatinine levels at 1-, 3-, 6-, 9-, or 12-month posttransplant between the two groups (P = not significant) (Fig. 1). The 1 year acute rejection rates in HBsAg-positive recipients and HBsAg-negative recipients was 38.8% and 28.0%, respectively, but there was no statistically significant difference between the two groups (P = 0.197). Infection complications in 1-year posttransplant are shown in Table 2. However, the difference in the incidence of infections between the two groups did not achieve statistical significance.
We compared the death-censored graft survival rates between HBsAg-positive recipients and HBsAg-negative recipients. The 1-, 3-, and 5-year death-censored graft survival rates of HBsAg-negative recipients were 98.2%, 96.7%, and 94.3%, respectively, and those graft survival rates of HBsAg-positive recipients were 100%, 100%, and 94.7%, respectively. There was no statistical difference between the two groups (P = 0.398) (Fig. 2). Only one of the 42 HBsAg-positive patients experienced graft rejection and resumed dialysis. Graft loss was due to chronic rejection.
Outcomes of posttransplant antiviral therapy
Most patients (n = 35, 83.3%) received lamivudine after kidney transplantation and the other patients received adefovir (n = 1) or entecavir (n = 6); these antiviral agents were started in patients with detectable HBV DNA or as preemptive therapy in HBsAg-positive dialysis patients (Fig. 3). During antiviral treatment, most of the patients (n = 35, 83.3%) were considered to have stable liver status and 7 patients had potential deterioration due to HBV reactivation and YMDD mutation. The 1-, 3-, and 5-year HBV reactivation-free survival rates were 95.0%, 82.6%, and 78.4%, respectively. Alternative or add-on therapies such as adefovir (n = 3) or entecavir (n = 4) were administered when HBV DNA titers rose and lamivudine resistance were detected. Five patients who received lamivudine showed lamivudine resistance, but liver functions were stable. Adefovir was used as a combination therapy with lamivudine in 3 patients and entecavir was replaced of lamivudine in 2 patients. The liver functions of patients who have HBV reactivation or YMDD mutation were well controlled by lamivudine and adefovir combination or entecavir switching.
All patients were under treatment with antiviral agents at the time of last assessment. Among these patients, only one was taking adefovir and lamivudine combination therapy and the others were on monotherapy. In the monotherapy group, 23 patients were treated with lamivudine, 6 with adefovir, and 12 with entecavir. At the end of follow-up, HBV reactivation was well controlled by switch or combination therapy in all patients with the disease. All patients were alive at the end of follow-up and none developed end-stage liver disease or hepatocellular carcinoma.
Comparison of kidney recipients with and without HBV reactivation
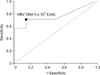
Baseline demographic and clinical characteristics of the two groups are shown in Table 3. ROC curve showed that the cutoff value of HBV DNA was 5 × 104 IU/mL (R2 = 77.1% and P = 0.025, respectively) (Fig. 4). The HBV DNA levels before transplantation in patients who experienced HBV reactivation were higher than in those who did not have HBV reactivation (median, 12 IU/mL; range, 11-4.25 × 106 IU/mL vs. median, 8.32 × 107 IU/mL; range, 12-2.92 × 108 IU/mL; P = 0.023) (Fig. 5). All patients with HBV reactivation had received lamivudine after transplantation, but the relative effectiveness of lamivudine (as compared to other drugs) on DNA levels or reactivation risk did not show statistical significance because only small numbers of patients received adefovir or entecavir. Multivariate analysis revealed that increased pretransplant HBV DNA levels (>5 × 104 IU/mL) were closely associated with HBV reactivation in HBsAg-positive recipients after kidney transplantation (hazard ratio, 1.559; 95% confidence Interval, 1.126-2.158; P = 0.007).
DISCUSSION
One important finding in our study was that treatment with antiviral drugs such as lamivudine, adevofir, and entecavir may suppress to nearby undetectable levels the viral activity in HBsAg-positive kidney transplant recipients. Among HBsAg-positive patients who did not receive preemptive treatments, the 10-year graft survival was significantly lower than in HBsAg-negative recipients [7]. However, HBsAg-positive recipients treated with lamivudine showed significantly higher 10-year graft and patient survival than HBsAg-positive recipients who did not receive antiviral treatments [8].
As compared to patients in previous series, the HBsAg-positive kidney transplant recipients in this study showed better patient and allograft survival [9,10]. In addition, there was no statistical difference in graft survival between HBsAg-positive recipients and HBsAg-negative recipients. At the end of follow-up, all patients were alive and only one patient experienced graft failure. We attribute these favorable outcomes to suppression of viral activities through antiviral treatments.
The use of immunosuppressive drugs enhances viral replication, which may accelerate liver injury and progression to liver failure in HBsAg-positive kidney transplant recipients [2]. The HBV genome contains a glucocorticoid-sensitive receptor. Glucocorticoid drugs increase activity at this receptor binding site and promote HBV transcription [11] followed by chronic HBV reactivation [12]. Our study revealed no deaths related to liver failure or portal hypertension; and this underscores the importance of sustained viral suppression in maintaining hepatic function and preventing acute-on-chronic hepatic failure even with concurrent immunosuppressive treatment.
Anti-HBV treatments, including pegylated interferon and antiviral agents such as lamivudine, adefovir, entecavir, or tenofovir, have changed the prognosis for HBV infection. Interferon cannot be used in renal transplant recipients because of its low effectiveness, direct nephrotoxicity and the associated risk of acute allograft rejection [13]. The first-generation antiviral agents lamivudine and adefovir effectively suppress HBV. Preemptive or prophylactic treatment of HBsAg-positive renal transplant recipients with lamivudine before hepatic dysfunction provides favorable short-term outcomes, including reduction in viral load, improvement in liver chemistry and prevention of irreversible histologic deterioration [2]. Prolonged use of lamivudine, however, may result in drug resistance. The most common mutation associated with lamivudine resistance involves the replacement of methionine by valine or isoleucine in the tyrosin-methionine-aspartate-aspartate (YMDD) motif of the HBV DNA polymerase (the "YMDD mutation") [14]. Genotypic resistance can be detected in 14%-32% of immunocompetent patients with chronic hepatitis B after one year of lamivudine treatment [15], increasing to 60%-70% after 5 years [16]. Thus, development of lamivudine resistance limits long-term use of the drug. The second-generation antiviral agents entecavir and tenofovir show higher antiviral potency than lamivudine and adefovir, and less tendency to induce mutation that results in drug resistance. By international consensus, these drugs are now recommended as first line therapies for HBV infection [17]. As antiviral therapies for HBV become increasingly effective, the prevention of HBV-related hepatocellular failure in HBV-infected renal transplant recipients becomes more certain. Based on findings here, we hypothesize that entecavir may be more effective in this situation than currently thought, because all patients with HBV reactivation received lamivudine and the entecavir-treated patients did not experience HBV reactivation; however, we could not test this possibility in this very small study. The efficacy of Entecavir in HBV-infected kidney transplant recipients should be further investigated.
Factors associated with increased risk of HBV reactivation include drug-resistant HBV [14,15,16] and high HBV DNA levels at the time of transplantation [18,19]. In this study, increased HBV DNA levels before transplantation were related to HBV reactivation afterwards. Thus HBsAg-positive patients awaiting kidney transplantation should receive antiviral therapy as increased HBV DNA level (≥5 × 104 IU/mL) to suppress HBV DNA to undetectable levels. This may greatly reduce risk for HBV reactivation after transplantation.
The limitations of our study include a retrospective design, a very small number of HBsAg-positive recipients to provide data. But given the high liver-related morbidity and mortality associated with rapid viral replication in conjunction with immunosuppressive therapy, a randomized controlled study that included HBsAg-positive renal transplant recipients without antiviral treatment would be unethical. Thus we compared HBsAg-positive recipients with HBsAg-negative in our data.
In conclusion, the development and application of potent antiviral agents has significantly increased graft and patient survival among HBV-infected recipients, although liver failure still occurs more frequently in this group compared with uninfected patients. This study showed that effective viral suppression in HBsAg-positive renal transplant recipients using antiviral agents improves both patient and allograft survival.






 XML Download
XML Download