

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Bronchogenic cysts are benign congenital anomalies related to the abnormal budding of the tracheobronchial tree during embryological development [1,2]. Most bronchogenic cysts occur in the mediastinum or within the pulmonary parenchyma, whereas cysts in the thyroid or perithyroidal area are rare [3]. Since many adults with bronchogenic cysts do not experience any symptoms, the cysts are often detected incidentally during the diagnosis of other diseases [4]. Although symptomatic bronchogenic cysts should be excised, the treatment of asymptomatic cervical bronchogenic cysts remains unclear [5]. Cystic lesions in the neck include branchial cleft cysts, thyroglossal duct cysts, bronchogenic cysts, thymic or thyroid cysts, and metastatic lymph nodes [6]. Cystic degeneration is also common in metastatic lymph nodes associated with thyroid cancer [7,8]. Metastatic lymph nodes affect the extent of lymph node dissection, especially in the lateral neck region. Therefore, correctly diagnosing cystic lesions in the neck is important for thyroid cancer surgery. However, benign bronchogenic cysts appear similar to metastatic lymph nodes, both by preoperative imaging and intraoperative field findings. The aim of this study was to review the clinical characteristics and proper management for cervical bronchogenic cysts that mimic metastatic lymph nodes during thyroid cancer surgery.
METHODS
Of the 18,900 patients treated for thyroid cancer at the Thyroid Cancer Center, Gangnam Severance Hospital, Younsei University College of Medicine, between January 2007 and April 2012, 18 patients (3 males, 15 females; mean age, 52.6 years) with bronchogenic cysts confirmed by postoperative pathologic examination were retrospectively reviewed in this study. Preoperative neck ultrasound and CT were performed for thyroid evaluation, and thyroid cancer was confirmed by fine needle aspiration cytology. Extent of thyroidectomy and lymph node dissection was determined using American Thyroid Association guidelines [9]. This retrospective study was approved by the Institutional Review Board of Gangnam Severance Hospital, Younsei University College of Medicine, Seoul, Korea.
RESULTS
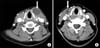
Of the 18,900 patients who underwent thyroid cancer surgery, 18 (0.1%) were confirmed as having cervical bronchogenic cysts; their clinical characteristics are shown in Table 1. All cervical bronchogenic cysts were asymptomatic, and cystic lesions were found during either preoperative diagnostic evaluation or thyroid cancer surgery. The mean size of the cervical bronchogenic cysts was 1.2 cm (range, 0.3 to 3 cm). Eleven cysts were located in the right paratracheal area, 3 in the left paratracheal area, and 1 each in the left thyroid cartilage, left inferior thyroid, right level III region, and anterior mediastinum. Fifteen patients underwent bilateral total thyroidectomy, whereas three underwent less than total thyroidectomy. All patients underwent central compartment node dissection, including cystic mass removal. None of these patients had any postoperative complications. Metastatic lymph nodes associated with thyroid cancer were found in five patients. Patient 4 was a 55-year-old female with an asymptomatic soft mass in the neck (Table 1). CT showed a homogeneous cystic mass that measured 3 cm × 1.5 cm around the thyroid cartilage (Fig. 1A). Although it was initially diagnosed as either a thyroglossal duct cyst or a metastatic lymph node with cystic degeneration, postsurgical analysis determined that it was a cyst lined with pseudostratified, ciliated, columnar epithelium containing underlying seromucinous glands. CT of patient 15 showed a 1.5-cm-sized cystic mass at the right level III region in the neck (Fig. 1B). The cystic mass was excised during thyroidectomy and was identified as a bronchogenic cyst (Fig. 2). Of these 18 patients, 15 did not have any abnormal radiological findings, except for lymphadenopathy during preoperative evaluations. Cervical bronchogenic cysts were less than 1.5 cm in size and were detected around the paratracheal area. Although these cysts resembled central lymph nodes in operative field analyses, final pathologic examinations identified them as bronchogenic cysts.
DISCUSSION
The tracheobronchial tree, which consists of the ventral trachea and the dorsal esophagus, is formed during the fifth week of embryogenesis. Bronchogenic cysts are often caused by an abnormal budding of the primitive foregut's tracheobronchial tree. When the connection with the tracheobronchial tree is lost, the bronchial buds may migrate to an aberrant position [1,10]. Bronchogenic cysts have been classified according to their site of origin: paratracheal, carinal, hilar, paraesophageal, and atypical (such as diaphragmatic, abdominal, intracutaneous, or subcutaneous, or in the supraclavicular neck area) [11].
Abnormal budding during tracheal development can cause bronchogenic cysts to form on the midline of the upper neck. However, cysts may also develop in the lower and lateral portions of the neck, if abnormal budding occurs during bronchial system development [12]. The thyroid and paratracheal regions are more frequently affected than the supraclavicular region and suprasternal notch, and the majority of cysts are midline [13]. In our study, 16 of the 18 cysts were detected around the thyroid and paratracheal areas, with the right paratracheal area more frequently affected, but we could not find any connection with the trachea.
Bronchogenic cysts in the cervical area are usually asymptomatic and are often detected incidentally through diagnostic evaluation of other diseases. Large cysts may cause dyspnea, respiratory distress, cough, and dysphagia in some individuals. Occasionally, secondary infection may occur, resulting in sinus tract formation, external drainage of purulent material if the cyst is superficial, or abscess formation if the cyst is deep [14]. The majority of intrathoracic bronchogenic cysts can be detected by chest x-rays, but these have little diagnostic value for cysts located in the neck [15]. CT provides a more accurate localization of these lesions, showing that typically they are round, fluid-filled, well-circumscribed masses of varying densities. Barium studies have also demonstrated abnormal communication of the respiratory tract with the esophagus or stomach [4]. However, definitive identification of these cysts can only be achieved by histopathological examination. Bronchogenic cysts are characterized by a pseudostratified, ciliated, columnar epithelial lining with underlying seromucinous glands [16]. Cervical bronchogenic cysts should be examined to differentiate them from branchial cleft cysts, thyroglossal duct cysts, thymic and thyroid cysts, dermoids and lymphangiomas, cystic hygromas, teratomas, and cystic neuromas [6]. Thyroglossal duct cysts and branchial cleft cysts are more common congenital abnormalities initially seen in the upper triangles of the neck [17]. Branchial cleft cysts are usually located high and lateral, whereas thyroglossal duct cysts are typically located midline on the anterior portion close to the hyoid bone. Bronchogenic cysts should also be distinguished from metastatic lymph nodes associated with thyroid cancer. Cystic degeneration is a common feature of metastatic lymph nodes associated with thyroid cancer [7,8]. Furthermore, the presence of metastatic lymph nodes affects the extent of lymph node dissection, especially in the lateral neck, and postoperative radioactive iodine therapy. In our study, we could not differentiate them from lymph node metastasis or other cystic lesions in preoperative imaging study or intraoperative features. Of these 18 patients, 15 did not have any abnormal radiological findings, except for lymphadenopathy and these cysts resembled central lymph nodes in operative field analyses. After the patients underwent thyroidectomy and central compartment node dissections, which included cystic mass removal, the bronchogenic cysts were identified via pathologic examination. If we had measured level of thyroglobulin (Tg) in fine-needle aspirate wash-out (FNA wash-out Tg) for the cystic lesion before surgery, that could be helpful for differential diagnosis. However unfortunately, we had not measured FNA wash-out Tg.
Management of asymptomatic cysts in adults remains controversial. Although continued observation has been suggested [18], recent studies recommend surgical excision to prevent infection, rupture, compressive symptoms, and malignant degeneration [2,12,13,19]. Our results showed that many bronchogenic cysts resemble metastatic lymph nodes and therefore required removal, dissection, and examination to be identified correctly. Furthermore, several case studies have indicated that carcinomas can develop from bronchogenic cysts, emphasizing the importance of complete surgical excision. Mucoepidermoid carcinomas arising from bronchogenic cysts have been reported in the thymus of a 59-year-old Japanese woman [20] and in the thyroid of a 44-year-old woman [21]. In addition, a recurrent malignant melanoma arising from a cutaneous bronchogenic cyst in the left scapular area has been reported in a 46-year-old Japanese man [22], and a poorly differentiated adenocarcinoma arising from a bronchogenic cyst in the cervical region was recently described [23]. Although cervical bronchogenic cysts are rare and benign, they should be distinguished from other cystic cervical masses, especially metastatic cervical lymph nodes associated with thyroid cancer. Furthermore, possible cervical bronchogenic cysts found during thyroid cancer evaluation or surgery should be surgically excised.


 XML Download
XML Download