

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Thyroid cancer is the most common cancer and breast cancer is the second-most common cancer in Korean women [1]. Many studies have evaluated the association between these cancers, which are both more common in women. Furthermore, the incidence of autoimmune thyroiditis, including Hashimoto's thyroiditis, is several fold higher in breast cancer patients than in control subjects [2,3,4, 5]. Hashimoto's thyroiditis was reported in 13.7% of breast cancer patients and in 2% of controls [3]. In another study, the odds ratio (OR) of autoimmune thyroiditis was 2.92 (95% confidence interval [CI], 2.13-4.01) in breast cancer patients, and the OR of the presence of antithyroid antibodies was 2.02 (95% CI, 1.63-2.50) [5]. In the same study, the risk of developing thyroid goiter was twofold higher in breast cancer patients than normal controls (OR, 2.26; 95% CI, 1.39-3.69) [5].
Epidemiologic studies have shown breast cancer patients have an elevated risk of developing thyroid cancer and vice versa [6,7,8,9]. The risk of thyroid cancer following breast cancer was increased by 31%-73% and that of breast cancer following thyroid cancer by 21%-89% [6,7,8]. Furthermore, the presence of breast cancer in thyroid cancer patients aged 40-50 years was found to be three times more likely than in age-matched controls [9]. In addition, a study that evaluated relations between the risk factors of breast cancer and thyroid cancer showed the incidence of thyroid cancer was 2.5 folds higher in women weighing over 60 kg [10].
A relationship between thyroid cancer and breast cancer was first postulated over 30 years ago, and thus, we considered an investigation of the characteristics of thyroid cancers occurring in breast cancer patients would aid prognostic predictions and treatment options. Accordingly, we investigated the clinicopathologic characteristics of thyroid cancer in breast cancer patients and compared these characteristics with those of thyroid cancer patients without breast cancer with respect to prognosis and treatment methods.
METHODS
One hundred and one patients diagnosed with breast cancer and thyroid cancer between January 1993 and September 2012 (the BT group) were enrolled in this retrospective comparative study. The patients received a diagnosis of thyroid cancer between August 1998 and September 2012 and of breast cancer between January 1993 and July 2012. These patients underwent a breast cancer operation in our institute or another hospital, but all were followed at our institute. Thyroid cancer was diagnosed before, after, or at the same time as breast cancer. All thyroid cancer operations were performed at our institute.
The control group (the oT group) was composed of 193 female patients that underwent a thyroid cancer operation between January 2008 and December 2008 at our institute. This timing was chosen because 2008 was the median time of thyroid operations in the BT group (from August 1998 to September 2012).
Thyroid lobectomy and isthmectomy with ipsilateral central lymph node (LN) dissection were performed for unilateral thyroid tumors (<1 cm in maximum diameter) suggestive of malignancy by fine-needle aspiration cytology when there was no suspicion of a nodule in the contralateral lobe. We also performed total thyroidectomy with bilateral central LN dissection. Levels II-V were routinely dissected during lateral neck LN dissection in thyroid cancer patients.
In patients with a tumor size of <1 cm, endoscopic thyroid surgery was performed using an axillary approach for patients that requested an endoscopic operation. Postoperative radioactive iodine (RAI) ablation was planned for patients with LN metastasis, distant metastasis, or TNM stage T3/T4, with consent. Follow-up studies comprised routine cervical ultrasonography (USG), a thyroid function test, CT, and positron emission tomography, if needed. At six months and one year postoperatively, cervical USG and a thyroid function test were performed, and subsequently, a semiannual thyroid function test and annual cervical USG were performed.
Our Institutional Review Board approved this retrospective study before the patient list was retrieved from the hospital database. Medical records, pathology reports, operation records, and radiological findings suggestive of recurrence or disease-related mortality were retrospectively evaluated.
Pearson chi-square test, Fisher exact test, and the independent t-test were used to evaluate differences between the BT and oT groups. In addition, Cox regression analysis and multivariate logistic regression analysis were performed. Statistical significance was accepted for P values of <0.05.
RESULTS
Clinicopathologic results for the 294 study subjects and the 101 thyroid cancer patients with breast cancer
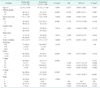
The clinicopathologic characteristics of the 294 study subjects are summarized in Table 1. Mean patient age was 48.6 years and papillary thyroid cancer (PTC) was the most common. Mean tumor size was 1.27 ± 1.03 cm, and the mean number of malignant thyroid tumors per patient was 1.47 (range, 1-11). Total thyroidectomy was performed in 76.9% of patients, and lateral LN dissection in 6.8%. Conventional open thyroidectomy was performed in 268 cases (91.2%) and endoscopic thyroid surgery in 26 (8.8%). The mean antithyroid peroxidase antibody level was 8.21 units/mL (range, 0.02-78.73 units/mL), and the mean antithyroglobulin antibody level was 9.50 units/mL (range, 0.01-102.29 units/mL). Mean follow-up duration was 40.78 ± 22.09 months.
In the BT group, mean age at thyroid cancer diagnosis was 51.4 years and mean age at breast cancer diagnosis was 48.7. Breast cancer was diagnosed before thyroid cancer in 83 patients (82.2%) and 14 patients (13.9%) were simultaneously diagnosed with thyroid and breast cancer. Mean time elapsed between the two operations was 35.53 ± 37.91 months (range, 0-207 months). In cases in which the primary disease was breast cancer, the interval between the two operations was 41.17 ± 38.41 months (range, 1-207 months), and in cases in which the primary disease was thyroid cancer, the interval between the two operations was 43.00 ± 26.92 months (range, 6-67 months). Breast conserving surgery was performed in 56/101 (55.4%) and modified radical mastectomy was performed in 45/101 (44.6%). Endoscopic thyroid surgery was performed in 13 cases (12.9%).
Differences between the clinicopathologic characteristics of patients in the BT and oT groups
Table 2 summarizes differences between the BT and oT groups. Mean tumor size was smaller in the BT group, and extrathyroidal extension was observed less often in the BT group. Mean age at thyroid cancer diagnosis was greater in the BT group. T stage was earlier and LN metastasis was less frequent in the BT group than in the oT group. The frequency of postoperative RAI ablation was analyzed in athyroid patients with follicular cell-derived cancer, and postoperative RAI ablation was performed significantly less often in the BT group (P < 0.001).
Evaluation of prognosis in the BT group and the oT group
Of the 294 study subjects, local recurrence (cervical LN or contralateral lobe recurrence) occurred in 12 patients (4.1%), distant metastasis occurred in 1 (0.3%), and one patient died from anaplastic thyroid cancer. In the BT group, no local recurrence or distant metastasis of thyroid cancer was observed. To reduce the possibility of confounding the analysis, we excluded non-PTC patients, which reduced the cohort to 281 patients. Thyroid cancer recurrence or thyroid cancer-related mortality occurred only in the oT group (0.0% vs. 6.1%, P = 0.009) (Table 3). Chi-square analysis showed that the presence of breast cancer, age, extrathyroidal extension, T/N stage, and follow-up duration were significantly related to recurrence. However, Cox regression analysis failed to identify any variable (including BT/oT group) significantly related to recurrence (data were not shown).
Factors affecting the performance of postoperative RAI ablation
Of the 227 athyroid patients with follicular cell-derived cancer, we excluded 3 patients that underwent breast surgery more than 6 months after thyroid surgery. Therefore, we analyzed the performance of RAI ablation in 224 patients. 146 patients were treated by postoperative RAI ablation (Table 4). In the BT group, postoperative RAI ablation was performed less often than in the oT group. In univariate analyses, RAI ablation was associated with younger age and larger and more invasive tumors. Multifocality, bilaterality, T stage, N stage, and TNM Stage were associated with the adoption of postoperative RAI ablation. Multivariate analysis indicated that the presence of breast cancer and N stage were associated with the adoption of RAI ablation. The OR of LN metastasis following postoperative RAI ablation was 11.851, and the OR of breast cancer in patients treated by RAI ablation postoperatively was 0.235.
DISCUSSION
Many studies have been performed to evaluate the relationship between breast cancer and thyroid cancer. Estrogen probably influences the physiology and pathology of thyroid glands, and 17β-estradiol is a potent mitogen of benign and malignant thyroid tumor cells [11,12,13]. Sodium/iodide symporter (NIS), which is located on the basolateral membrane in normal thyroid and lactating mammary glands, mediates iodide uptake by the thyroid gland and lactating breasts. Furthermore, basal NIS gene expression is detected in approximately 80% of breast cancer specimens, although the fraction exhibiting functional iodide transport is relatively low [14]. Moreover, abundant TSH receptors are present in breast tissue [15,16], although the role of TSH in the regulation of NIS in breast cells remains controversial [3,17]. Radiation therapy has been considered to contribute to the development of breast and thyroid cancer. Based on an analysis of data obtained from the National Cancer Institute's Surveillance, Epidemiology and End Results database, Chen et al. [18] reported that women with a history of thyroid carcinoma, particularly premenopausal white women, have a greater than expected risk of developing breast carcinoma, and suggested that RAI therapy for thyroid cancer potently contributes to breast cancer development. Rubino et al. [19] suggested that high radiation doses increase the risk of second malignancies, including thyroid cancer, slightly after breast cancer treatment.
However, Huang et al. [20] concluded that women administered external beam radiation therapy for breast cancer, are not at increased risk of developing thyroid cancer. In fact, after a 10-year follow-up, the relative risk of radiation-associated thyroid cancer after initial external beam radiation therapy for breast cancer was 1.0 (95% CI, 0.7-1.5). In another study that evaluated the influence of external beam radiation therapy for breast cancer on thyroid cancer development, and the influence of RAI therapy for thyroid cancer on breast cancer development, no relationship was found between radiation dose and the risk of thyroid cancer after radiation therapy in breast cancer patients or vice-versa [21]. Therefore, although radiation therapy has been considered to contribute to the development of thyroid cancer or breast cancer after external beam radiation therapy or RAI therapy, no reliable data is available on the topic.
The correlation between breast cancer and thyroid cancer may not indicate causality, because the increase in the observed incidence of thyroid cancer may be the result of increased medical surveillance for breast cancer [22]. However, Park et al. [23] reported that 518 patients with breast cancer showed a relatively high (2.5%) incidence of thyroid cancer. In another report, the same authors compared incidences of thyroid cancer in breast cancer and routine screening patients. Thyroid cancer was diagnosed in 1.9% of breast cancer patients (13/685) and in 0.6% of routine screening patients (29/4864), which represented a significant difference (P < 0.05). Thus, it was concluded that breast cancer patients might have some internal factors that influence thyroid cancer development [24].
Few studies have been conducted on the characteristics of thyroid cancer in breast cancer patients. Park et al. [24] reported different features for thyroid cancer in patients with or without breast cancer. In particular, LN metastasis was more prevalent in thyroid cancer patients without (13/29, 44.8%) than in those with breast cancer (2/13, 15.4%). Shin et al. [25] performed a study on the characteristics of thyroid cancer with or without breast cancer; almost all breast cancer patients with thyroid cancer were diagnosed with PTC. The authors found that tumor size was significantly smaller in patients in thyroid cancer patients with breast cancer than in thyroid cancer patients.
In our series, the BT group had a smaller mean tumor size and a lower prevalence of LN metastasis, which concurs with previously published data. In addition, extrathyroidal extension was less prevalent and T stage was less advanced in the BT group. Furthermore, all patients in the BT group were diagnosed with PTC. Although we could not conclude what is the exact cause of earlier status in BT group, we considered that it was because of medical surveillance.
To our knowledge, this is the first study to evaluate the prognosis of thyroid cancer in breast cancer patients. Initially, we expected that BT group would be found to show a more favorable prognosis than oT group due to an early disease status at diagnosis. The chi-square test showed that the BT group showed a more favorable prognosis than the oT group, as neither recurrence nor thyroid cancer-related mortality were observed in the BT group. The other factors related to prognosis were age, extrathyroidal extension, and T/N stage, which are known prognostic factors in thyroid cancer. However, Cox regression analysis failed to reveal any factors significantly related to recurrence in our series, which we believe was due to different follow-up durations and the small number of patients that experienced recurrence. If in fact, the prognosis of thyroid cancer in patients with breast cancer is more favorable than in patients without breast cancer, thyroid USG would be helpful to identify second malignancy in breast cancer patients, as the early detection of thyroid cancer improves prognosis.
This is the first series to investigate treatment method in thyroid cancer patients with breast cancer. Interestingly, postoperative RAI ablation was performed less often in the BT group than in the oT group. Our comparison of group characteristics (Table 2) showed that in the BT group, 41.9% of patients received postoperative RAI ablation, whereas in the oT group 75.2% of patients were treated with RAI. Although we believed this difference might be related to an earlier T stage and less LN metastasis, this analysis revealed a factor not previously associated with the performance of postoperative RAI ablation. Finally, the presence of breast cancer and N stage were found to be positively associated with the performance of RAI ablation.
The OR of the BT group versus the oT group for postoperative RAI ablation was 0.235. This reduced usage of RAI ablation in the BT group was ascribed to the following. First, breast cancer patients treated with chemotherapy or radiotherapy sometimes refuse to undergo RAI ablation. Second, thyroid cancer is treated as a less grave disease than breast cancer by doctors and patients. Third, doctors try to avoid patient suffering caused by additional treatment. Forth, chemotherapy and radiotherapy can both prevent the administration of RAI at optimal ablation times. Although RAI ablation was not found to be a significant prognostic factor for thyroid cancer in our series, this result is interesting.
We have found that endoscopic thyroid surgery can be used to treat patients with breast operation scars, who are commonly reluctant to have another scar in the neck area. Our patients were operated on using an axillary approach for endoscopic thyroid surgery; however, a bilateral axillo-breast approach can also be used. Both of these endoscopic surgeries are performed through the subcutaneous layer in the anterior chest and do not affect breast tissue. When the bilateral axillo-breast approach is used for endoscopic thyroid surgery, breast tissue can be used as a buffer during instrument manipulation. Furthermore, because endoscopic thyroid surgery can be performed in male patients using a bilateral axillo-breast approach, thyroid cancer patients who have undergone mastectomy can also be operated on using endoscopic thyroid surgery.
In conclusion, thyroid cancer patients with breast cancer had smaller tumors, and less frequently had extrathyroidal extension or LN metastasis. However, no significant prognostic difference, including recurrence and mortality, was observed between the BT and oT groups, which we presume was due to different follow-up durations and small numbers of recurred patients. Thus, we believe that a study with a longer follow-up duration and a large number of patients should be conducted to determine whether the prognoses of thyroid cancer patients with or without breast cancer differ. Furthermore, the study shows thyroid cancer patients with breast cancer underwent RAI ablation less often, and demonstrates that endoscopic thyroid surgery can be used to treat these patients.



 XML Download
XML Download