

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Nipple discharge is rare in infancy, except for physiologic discharge in newborns. Furthermore, bloody nipple discharge in children is extremely rare; fewer than 30 cases have been reported worldwide. Mammary duct ectasia is the most common cause of bloody nipple discharge in children; however, its etiology and pathophysiology remain unclear. Therefore, it is difficult to predict the clinical course of this condition and to make medical management decisions.
Here, we report a 14-month-old boy who exhibited unilateral mammary duct ectasia with bloody nipple discharge.
CASE REPORT
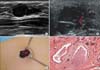
A 14-month-old boy exhibited a mass in the right breast with bloody nipple discharge for 2 weeks before presenting a our hospital. There were no abnormalities in the patient's medical, familial, or developmental histories or in the maternal medical history. On physical examination, a 1-cm palpable mass without tenderness was noted in the subareolar region of the upper right breast. When the mass was squeezed, dark brown nipple discharge appeared (Fig. 1). There were no signs of inflammation in the physical examination or laboratory findings.
An ultrasonogram revealed a 1.0 cm × 0.8 cm multiseptated cystic mass in the right subareolar region. The macrocystic portion of the mass exhibited internal echogenicity. Minimal septal vascular flow was noted, and the mass was thought to be a complicated hemorrhagic lymphangioma or mammary duct ectasia (Fig. 2A, B).
Surgical excision was performed via a circumareolar incision, and a dark, bloody, fluid-filled cystic mass was removed. The mass, which was connected to main duct, was completely excised (Fig. 2C).
The pathologic diagnosis was mammary duct ectasia. A microscopic analysis of the specimen demonstrated multiple dilated ducts with periductal fibrosis. The lumens of the dilated ducts contained histiocytes and degenerated epithelial cells, and duct stasis was observed (Fig. 2D).
DISCUSSION
Breast nipple discharge is common among adult females; it may manifest as a milky or bloody discharge and may be physiologic or pathologic. The most common cause of breast disease with bloody nipple discharge in adults is intraductal papilloma, with an incidence of 2%-3%.
Possible causes of bloody nipple discharge in children include benign conditions such as an abnormal response of the breast tissue to maternal hormones, high levels of progesterone, mammary duct ectasia, intraductal papilloma, intraductal cyst, or mammary ductal hyperplasia. Rarely, prolactinoma or inflammatory breast pathologies such as mastitis lead to childhood bloody nipple discharge, and trauma and infantile gynecomastia are additional causes [1,2].
The pathogenesis and etiology of mammary duct ectasia with bloody nipple discharge are unclear. According to a recent review of 23 cases of mammary duct ectasia in children [3], there is a 10:4 ratio of males to females, and the average age is 38 months. In contrast, mammary duct ectasia is rarely found in adult men, which implies that mammary duct ectasia in children has a different developmental cause from the adult forms. The extremely early onset of the disease in a 2-month-old child suggests the importance of an association between the pathophysiology of mammary duct ectasia and developmental abnormalities or a maternal history of abnormal hormones or medication, especially when a breast-feeding child is affected [4].
There have been some reports of bacterial growth in the nipple discharge [5,6], although there was a lack of clinical or histological inflammatory evidence in our case. It is reasonable to assume that such bacterial growth might be due to a secondary bacterial infection or contamination.
When a child presents with bloody nipple discharge visits, a sufficient clinical history, including the birth, feeding history, and maternal/medical history should be taken. Laboratory examinations including complete blood cell count, coagulation test, hormonal profile, discharge culture, Gram staining, and noninvasive imaging studies such as ultrasonography should be performed.
The ultrasonographic findings of mammary duct ectasia include tubular anechoic structures or dilated ducts filled with debris. The cystic lesions may be small and simple, or larger and multiseptated or complex [7,8]. The Cystic appearance on ultrasound may lead to alternate differential diagnoses. Our case was preoperatively diagnosed as complicated lymphangioma with hemorrhage, and the differential diagnosis was mammary duct ectasia.
According to the literature, surgeons tend to choose surgical excision without observation like this case. However, mammary duct ectasia with bloody nipple discharge has been reported to resolve spontaneously within 3-9 months [1,9,10]. Therefore, invasive therapy for a cystic mass with bloody nipple discharge in a child should be considered carefully because it might damage the normal, developing bud tissue. Although the optimal duration of follow-up and timing of surgical excision have not yet been established, conservative therapy coupled with relief for parental anxiety should be considered first when a child presents with a cystic mass with bloody nipple discharge.

 XML Download
XML Download