

 ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Pilonidal sinus (PS) is a common chronic, benign disease of young adulthood. It is more commonly encountered in males than in females. Although several anatomical localizations may occur, it is most frequently seen in the sacrococcygeal region. When left to its natural course, it results in localized inflammation with occasional abscess formation causing fistulae, sinus development, and chronic inflammation in the presacral region. Although it was first described as a congenital disease, it is currently known to be an acquired condition [1,2].
PS is not considered to be a major problem in terms of surgical techniques. However, considering the gender and age group it mainly affects, it is a serious condition that can cause a significant reduction in labor and a disruption of the educational process in every community [3]. Therefore, when evaluating the effectiveness of treatment, resumption of daily activities (time off work) is a parameter that is at least as important as the rate of recurrence.
We investigated whether there is a factor that can aid determination of the preferred technique by comparing the early and late results of two different surgical techniques for the treatment of PS.
METHODS
The records of patients who underwent surgery between 2001-2009 in the Department of General Surgery of Sakarya University School of Medicine and Afyon Kocatepe University School of Medicine with a diagnosis of primary-recurrent or complicated PS were retrospectively reviewed. The medical records of 213 patients in whom Limberg flap (LF) or V-Y flap techniques were applied for reconstruction after the excision were evaluated retrospectively.
A total of 37 patients who had diabetes mellitus, were using steroid therapy on a regular basis for several reasons, had bilateral flaps, had multiple recurrent disease, and were undergoing no regular clinical follow-up were excluded from the study. The results of the remaining 176 patients were reviewed in terms of demographic characteristics, postoperative complications, hospital stay, resumption of daily activities, and duration and recurrence of disease.
All patients underwent operations in the prone position under spinal anesthesia, and a suction drain was placed in the operative field. Patients in both groups were not allowed to resume their work until they were free of discomfort and pain during normal daily activities.
Surgical procedures
All operations were performed by two surgical teams work ing in different clinics. Flap technique selection was made by the surgeon who performed the operations according to the defect size and his experiences. And, same flap tech niques were performed by the same surgeons (Limberg flap by A.F. and D.E.; V-Y flap by O.T. and A.G.).
For LF; the planned excision site and the site that would be used for reconstruction were marked with a marking pen, the cyst was excised with a rhomboid incision, and a LF was prepared from the right gluteal region. Hemostasis was achieved by electrocautery after the excision, followed by placement of an aspirative drain in the incision. The flap was sutured to the presacral fascia with absorbable sutures (2/0 Vicryl), the subcutaneous tissue was approximated with 3/0 Vicryl sutures, and the skin was closed using 3/0 Prolene mattress sutures (Fig. 1).
For V-Y flap; the planned excision site and the site that would be used for reconstruction were marked with a marking pen, the cyst was excised with an eliptic incision. V-shape fas ciocutaneous flap was prepared by going down to the gluteal fascia, and was moved towards the defect. Hemostasis was achieved by electrocautery after the excision, followed by placement of an aspirative drain in the incision. The V part of the flap was sutured to the presacral fascia with absorbable sutures (2/0 Vicryl), the subcutaneous tissue was approximated with 3/0 Vicryl sutures, and the skin was closed using 3/0 Prolene mattress sutures. Primary closure was performed for the opening in Y's leg (Fig. 2).
Patients had postoperative recurrent disease were treated with the same technique as the primary operation, using a flap from the contralateral gluteal region.
Wound separation was defined as the clinical situation comprising the consecutive stages of hyperemia, serous discharge, and dehiscence of the suture line, respectively. Wound infection was defined as purulent discharge from the incision line accompanied by microbiological growth in the wound culture. Flap necrosis was defined as complete necrosis of the flap, whereas localized areas of necrosis not exceeding a surface of 2 cm2 were included in wound separation. Develop ment of hematoma, wound separation, seroma, and wound infection were defined as minor complications, while flap necrosis was defined as a major complication. Wound separation was treated by daily wound dressings, and all patients recovered with secondary healing. Patients who developed wound infections were treated with parenteral antibiotics, daily dressings, and secondary suturing.
Postoperative hematomas were evacuated in the operating room under sterile conditions, and hemostasis was achieved. Seroma development was followed by a physical examination and was treated with ultrasound-guided aspiration on an outpatient basis.
A total of 13 variables were compared between the two groups. Student t test was used for comparison of continuous variables: lenght of hospital stay and time to feeling ready to return to work between the groups. Pearson χ2 test was used for comparision of age, sex and nominal variables: type of presentation (previous infection-abscess drainage-recurrence history). Fischer exact test was used for comparison of type of complications and recurrence rate between the groups. Stati stical analysis was performed using the SPSS ver. 10.0 (SPSS, Inc., Chicago, IL, USA), and a value of P < 0.05 was considered to indicate statistical significance.
RESULTS
The study included 165 males (93.7%) and 11 females (6.3%) with a mean age of 25.3 years (range, 16 to 70 years). Thirteen patients (7.3%) underwent operation due to recurrent PS. There were 90 patients in the LF group (group 1) and 86 in the V-Y flap group (group 2). None of the patients had signs of active inflammation or abscesses during the procedure. The distribution of patients in both groups according to demographic characteristics, duration of hospital stay, and resumption of work are given in Table 1.
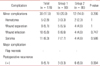
Minor complications (hematoma, wound separation, wound infection, and seroma) were observed in 5 (2.8%), 9 (5.1%), 10 (5.6%), and 11 (6.3%) patients, respectively, when all patients were examined. There were no major complications (i.e., the development of total flap necrosis). The distribution of complications within the groups is shown in Table 2.
In each group, there was one seroma developed patient for whom aspiration was necessary more than twice. In both patients, the clinical course after aspiration of the seroma was uneventful. Wound separation in two patients in group 1 and in one patient in group 2 was caused by tension of the wound edges and occurred secondary to wound infection in other patients.
The patients in group 1 were discharged 24 hours after the surgery, whereas the patients in group 2 were discharged after a mean of 4.4 days (2 to 6 days). Resumption of work was achieved after a mean of 17.1 days (13 to 21 days) in group 1 and 32.7 days (18 to 47 days) in group 2. There was no perioperative or postoperative mortality. During the average follow-up of 65 months (36 to 110 months), nine patients (5.1%) developed recurrent disease.
There were no differences between the two groups with respect to age (P = 0.212), gender (P = 0.483), presence of preoperative recurrent disease (P = 0.508), postoperative minor complications (P = 0.286), or development of postoperative recurrent disease (P = 0.094), whereas resumption of daily activities was longer in patients in group 2 (P < 0.001).
DISCUSSION
The ideal method of treatment for PS would be one with minimal tissue loss, minimal postoperative morbidity, excellent cosmetic results, rapid resumption of daily activities, low cost, and a low recurrence rate [4]. However, although numerous ope ra tive and nonoperative treatment methods have been described, no treatment comprises all of these features.
The main technical difficulty of PS surgery is not ex ci sion of the cyst along with all of the sinuses, but rather reconstruction of the remaining defect. The excision with open packing technique is associated with a long recovery period [5]. Although the primary closure method is known to result in rapid recovery with a rapid resumption of daily activities, high complication and recurrence rates have been reported [6-8]. The reasons for the negative results of the primary closure method are the incision scar in the midline, the inability to flatten the natal cleft, and the tissue tension. Various techniques have been described that attempt to eliminate the fac tors that cause these negative results of primary closure, resulting in lower recurrence rates [9-13].
Flap techniques in the surgical treatment of chronic sacrococcygeal PS have become the treatment of choice due to decreased relapse rates associated with flattening of the natal cleft, healing without tissue tension, and satisfactory cosmetic results [14].
The LF, which is one of the most common techniques, is associated with wound infection, seroma, wound separation, flap necrosis, and recurrence rates of 0.8-7.6%, 1.5-5.2%, 0-4.1%, 0-3%, and 1.2-4.9%, respectively, in the literature [3-7,14-17]. In our LF results agreed with previous reports.
The V-Y flap, which was first described by Khatri et al. [18] in 1994 for the recurrence of PS in five patients, is currently used in the treatment of PS with wide excision or recurrent disease. In the literature, the rates of wound infection, seroma, wound separation, and recurrence after the V-Y flap were reported to be 0-6.7%, 0-8.5%, 0-18.1%, and 0-11.1%, res pectively [16,19,20]. In our V-Y flap results agreed with previous reports.
In our study, the complication rates in both groups were con sistent with those reported in the literature. In addition, comparison of the two groups showed no difference in terms of complications or recurrence (P = 0.286 and P = 0.094, respectively). In their study of 111 patients, Unalp et al. [16] compared the LF with the V-Y flap and found that although there were no significant differences in terms of complications between the two techniques, the rate of recurrence was statistically significantly higher in the V-Y flap group. In our study, although there were more recurrences in the V-Y flap group, the difference was not statistically significant (P = 0.094).
PS is not considered to be a major problem in terms of surgical techniques. However, considering the gender and age group that it mainly affects, it is a serious condition that can cause a significant reduction in labor and disruptions in the educational process, especially in populations with a high incidence of the disease [1]. Therefore, when evaluating the effectiveness of treatment, resumption of daily activities at work (time off work) is a parameter that is at least as important as the rate of recurrence. Resumption of daily activities at work for the LF is reportedly as long as 12.4 to 18.8 days [3,14-17,21], whereas that of the V-Y flap is from 14.4 days to 4 weeks [16,20,22]. In our study, the time to resumption of daily activities was significantly longer in the V-Y flap group (P < 0.001). One of the reasons may be that V-Y flap have preferred in patients with more complicated.
In conclusion, various flap methods have been used to treat sacrococcygeal PS, and each is associated with different postoperative results and success rate. Many factors (such as: primary or recurrent disease, length of sinuses, defect size, patient preference, surgeon experience) are effective on flap technique selection. In this study were found that the early postoperative and long-term results of the LF and V-Y flap techniques were similar, however, V-Y flap had longer resumption of daily activities at work compared with the LF technique. Therefore, we think that the patient's employment (or position in working life) should also be considered when determining which technique to use.



 XML Download
XML Download