

 ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Thyroid cancer is the most common cancer in Korea [1]. Papillary thyroid cancer (PTC) is the most common but least aggressive histologic subtype of thyroid cancer. Most patients with PTC have an excellent prognosis. These excellent prognoses accentuate the lower complication rate of thyroid surgery and the improved postoperative quality of life. Many studies have evaluated the major complications of thyroidectomy, such as hypoparathyroidism and recurrent laryngeal nerve injury, but postoperative adhesive symptoms have been overlooked in those previous studies. Many patients complain of adhesive symptoms including swallowing difficulty or a pulling sensation during neck extension [2]. Moreover, internal adhesion scars after neck surgery are often externally visible (Fig. 1).
Numerous antiadhesive agents such as nadroparine calcium and aprotinin have been introduced. Barrier agents such as a sodium hyaluronatecarboxymethyl cellulose (HA-CMC) membrane (Seprafilm, Genzyme Co., Cambridge, MA, USA), HA-CMC solution (Guardix, Hanmi Medicare, Seoul, Korea), and an oxidized regenerated cellulose barrier (Interceed, Ethicon Inc., Somerville, NJ, USA) have also been used. The efficacy of these agents has been evaluated exclusively in the peritoneal and pelvic cavities. Studies on these agents have primarily focused on evaluating abdominal or pelvic pain, as well as intestinal obstructions and infertility [3-8].
An HA-CMC membrane (Seprafilm) was developed to reduce the formation of postoperative adhesions. Each chemical constituent in the solution has been shown to prevent the development of adhesion [9].
As far as we know, this is the first randomized double-blinded prospective study to evaluate the antiadhesive effect and safety of HA-CMC membranes in thyroidectomy.
METHODS
Patients
Between February and November 2011, 192 patients who underwent total thyroidectomy due to micro-PTC smaller than 1 cm, which was confined to thyroid tissue, were initially enrolled in this study. Age of patients ranges from 20 to 70. All operations were done by a specialized endocrine surgery team (Y.Y.K., L.K.E., C.J.Y.). The number of patients enrolled was calculated based on a previous study that had used a HA-CMC solution [2].
Patients were excluded if they had a history of previous neck surgery, radiation exposure, an uncontrolled medical illness causing swallowing difficulty like stroke or drug abuse. Following approval by the Institutional Review Board (IRB No. H-1011-009-338), all patients gave their written informed consent to participate in the study. The patients were randomized with 96 patients in both the study and control groups using a web-based randomized allocation protocol.
Twenty patients were dropped because of lateral lymph node dissection during the operation; 6 were dropped because of loss of follow-up in the outpatient department; 3 were dropped because their final pathologic reports were benign follicular neoplasm, and one patient was dropped as the patient's operation was cancelled due to the development of anaphylactic shock before the operation. Thus, finally, the study group and control group consisted of 80 and 82 patients, respectively. All patients and the examiner were blinded to the group allocation.
This system used a 4 × 6 random permuted block operated by the Medical Research Collaborating Center (MRCC), Seoul, Korea. Randomization was done after the completion of hemostasis and before closing the strap muscle with a double blinded method.
Antiadhesion
HA-CMC membranes (Seprafilm) are nontoxically denatured polysaccharides composed of hyaluronic acid and carboxymethyl cellulose. This material transforms to a hydrophilic gel in a wet environment within 48 hours and then functions as a protective coat for 7 to 30 days. HA-CMC membranes degrade within 1 month in vivo.
Each patient in the initial study group had a 7.5 cm × 13 cm HA-CMC membrane applied to the operative field: the thyroid bed, around the trachea, and the flapped area beneath the platysma (Fig. 2). Patients in the initial control group did not have the HA-CMC membrane applied. At 2 weeks, 3 months and 6 months postoperatively, complications including swallowing difficulty, wrinkles, and inflammation were assessed using 8 items (Table 1). Among these items, swallowing difficulty and wrinkles are items concerning the antiadhesive effect of the HA-CMC membrane, and inflammation is an item regarding the safety of the HA-CMC membrane. At each assessment, a physician who did not know the allocation of the patients examined the patients and described their scores on neck wrinkles.
Statistical analysis
Statistical analysis was performed using IBM SPSS ver. 18.0 (IBM Co., Armonk, NY, USA). A repeated measures analysis of variance (ANOVA) test was used to analyze the changes in complications between the different postoperative periods and to compare complications between the study and control groups at each postoperative time point. Continuous variables were expressed as the mean ± standard deviation, and statistical significance was defined as P < 0.05. MRCC provided advice on statistical analyses and illustration of graphs.
RESULTS
The clinical characteristics of the final 162 patients included in this study are presented in Table 2. The two groups were comparable with regard to sex, age, and operation time. There were no major complications such as bleeding, inflammation, aspiration, or dyspnea.
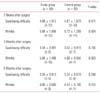
Table 3 presents minor complications such as swallowing difficulty and wrinkles. There were no significant differences between the study group and control group. The distribution pattern was not a normal variation; therefore, the repeated measures ANOVA test was used to analyze the changes in complications between different postoperative periods and to compare the complications between the study and control groups at each postoperative time point.
Table 4 presents the results of the repeated measures ANOVA test for swallowing difficulty and wrinkles, respectively. Both swallowing difficulty and wrinkles de creased over time (P < 0.0001), but use of the HA-CMC membrane was associated with neither swallowing difficulty nor wrinkles. There were no significant differences between the study and control groups. Fig. 3 shows these results for swallowing difficulty, and wrinkles.
DISCUSSION
The aim of this study was to evaluate the antiadhesive effect and safety of HA-CMC membranes in thyroidectomy. We showed that there was no significant difference in the total adhesion score between patients to whom the HA-CMC membrane was applied during surgery and the control group. This is believed to be the first prospective double-blinded randomized controlled study to evaluate the effects of HA-CMC membranes in thyroid surgery.
An ideal adhesion barrier should be degradable and not cause a foreign body reaction, impair wound healing, or promote infection [10]. To prevent contact between the injured areas, a barrier agent should remain effective for an adequate amount of time to allow reestablishment of the mesothelium [8].
Postoperative adhesion formation causes significant surgical morbidities such as intestinal obstruction, infertility, and complicated reoperations and continues to be an economic burden on the healthcare system [11,12]. Many factors, including trauma, ischemia, foreign material, and deposition of blood contribute significantly to the risk of postoperative adhesion formation [13,14]. Adhesion barrier devices that are used to separate tissue surfaces and prevent adhesions are an increasingly accepted adjunct to abdominopelvic surgery. Many studies have shown the antiadhesive effect of HA-CMC in animal models, human abdominal surgery, human facial surgery, human esophageal surgery, human breast surgery and human craniotomy [15-22]. Among them, there were interesting studies on a novel antiadhesive film based on cross-linked carboxymethylcellulose and atorvastatin, with that of sodium hyaluronate-carboxymethylcellulose [23,24]. They reported an equivocal or more improved antiadhesive effect of the novel material.
We speculated that the HA-CMC membrane did not have an antiadhesive effect in thyroid surgery because the membrane type antiadhesive material did not have a lubricating effect between the neck muscles. There is no natural barrier in the neck space in contrast to the abdominal cavity where the peritoneum functions as a natural barrier. In the abdominal cavity, membrane type antiadhesive materials may be enough to prevent adhesion between the peritoneum and bowel since the peritoneum may separate organs during healing. However in the neck space, both separation and lubrication could be necessary to prevent adhesion since there is no natural barrier like the peritoneum. Thus, the HA-CMC membrane may not be an ideal antiadhesive material in thyroid surgery compared to the HA-CMC solution. The HA-CMC solution showed a little antiadhesive effect although there was no significant effect [2].
There were no complications related to the application of the HA-CMC membranes in the study group. The HA-CMC membrane has been shown to be safe for use in abdominal or pelvic surgery, with respect to abscess formation, pulmonary embolism, and foreign body reactions. The HA-CMC membrane also did not have adverse effects on the oncological outcome of adjuvant therapy [7]. However, wrapping the sutures or staple line of a fresh bowel anastomosis should be avoided due to the increased risk of sequelae associated with anastomotic leakages [13]. Considering our results and the absence of such anastomosis in the operative field, it appears that the HA-CMC membrane is safe for application in thyroidectomies.
Most patients in the present study showed signs and symptoms of postoperative adhesion to some degree. Primarily as a result of the loss of normal tissue planes caused by postoperative adhesion, a second thyroid operation is associated with a high rate of complications, such as hypoparathyroidism and recurrent laryngeal nerve injury [25].
At present, there is no reliable method for measuring the adhesion grade, and we could not do anything other than use a questionnaire with a visual analogue scale, which is the limitation of this study.
Age may be an important factor to adhesion, so subgroup analysis was done with the cutoff value of age 50. However, there was no significant difference in subgroup analysis. The P-value of swallowing difficulty were 0.164 in age ≤50 group, and 0.963 in age >50 group. And the P-value of wrinkle were 0.872 in age ≤50 group, and 0.437 in age >50 group.
In conclusion, the present study shows that the signs and symptoms of postoperative adhesion after thyroidectomy are common but decrease over time. The application of an HA-CMC membrane in thyroidectomy is safe but the antiadhesive effect of HA-CMC membrane in thyroid surgery is still uncertain. Further investigation is needed to confirm the anti-adhesive effect of HA-CMC membrane in thyroid surgery.






 XML Download
XML Download