

 ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Central vein catheterization is a common practice for volume resuscitation, emergency venous access, parenteral nutrition, hemodialysis, and central venous pressure monitoring; especially for stable and long-term administration of chemotherapeutic agents, implantable central venous devices are placed through the internal jugular venous route or subclavian venous route.
As research on internal jugular venous access using real-time ultrasound has been conducted and widely accepted, the frequency of subclavian venous access has been reduced because of life-threatening complications such as hemothorax, pneumothorax, mediastinal hematoma, vascular perforation, and myocardial injury [1,2]. Therefore, reports on pinch-off syndrome that occurred occasionally in the past have recently become rare. The authors encountered pinch-off syndrome in 3 patients who had undergone totally implantable venous device insertion through the right subclavian route. We report on this rare but critical complication.
CASE REPORTS
Case 1
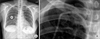
A 42-year-old woman with cancer of the left breast had undergone breast conservative surgery on January 4, 2011. An implantable venous port was inserted through the right subclavian vein for adjuvant chemotherapy, and the location was confirmed by chest radiography (Fig. 1). There was no problem with the catheter location, but a pinch-off sign showed as a catheter deviation between the clavicle and the first rib. After the initial injection of chemotherapeutic agent, the patient did not experience pain or swelling, and because there was no problem with blood aspiration or flushing, chemotherapy was administered 3 times under close observation. Three months after the port insertion, the patient was hospitalized for the fourth adjuvant chemotherapy. A chest radiograph showed that the transected catheter had embolized to the right atrium (Fig. 2). The patient was referred to an interventional radiologist, and the embolized catheter was successfully removed via the percutaneous approach through the right internal jugular vein under fluoroscopic guidance (Fig. 3). The remaining implantable venous port was removed surgically.
Case 2
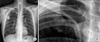
A 56-year-old woman with stomach cancer had undergone gastrectomy on December 31, 2007. After the operation, an implantable venous port was inserted through the right subclavian vein, and adjuvant chemotherapy was administered 6 times without any unusual complications. The patient had follow-ups on a regular basis, and the port was removed 18 months after its insertion. Part of the catheter was fractured and had embolized the right atrium and inferior vena cava, which was confirmed by chest radiography after the procedure (Fig. 4). In a retrospective review of the patient's chest radiographs, a pinch-off sign was noted in the chest radiograph taken immediately after the port insertion and the catheter's course was deviated by the clavicle (Fig. 5). During the adjuvant chemotherapy and outpatient follow-up observations, the patient did not complain of any pain or swelling, and there was no unusual problem with drug administration through the port. Transection of the catheter is assumed to have occurred at the end of the adjuvant chemotherapy, which was 6 months after the port insertion, but the exact time was impossible to confirm. The patient was referred to an interventional radiologist, and the embolized catheter was successfully removed by a percutaneous approach through the right internal jugular vein under fluoroscopic guidance (Fig. 6).
Case 3
A 48-year-old man with rectosigmoid colon cancer had undergone low anterior resection on July 15, 2011. For adjuvant chemotherapy, an implantable venous port was inserted through the right subclavian vein, and its location was confirmed by chest radiography (Fig. 7). No associated complication with the location of the catheter, and no pinch-off sign was suspected. The patient had undergone adjuvant chemotherapy 4 times without any unusual problems, ended the therapy of his own accord, and was lost to follow-up. Six months after he terminated the therapy, the patient returned to the outpatient clinic. His test results indicated that his disease had aggravated; therefore, chemotherapy was initiated again with different medications. He had chemotherapy twice during 2 months without any unusual complications but the port became dysfunctional after he was hospitalized for the third cycle; therefore, the removal of the original venous catheter and reinsertion through the left subclavian route were conducted. In the chest radiograph taken immediately after the second cannulation, some parts of the catheter of the removed right subclavian venous port remained (Fig. 8). In a retrospective review of the patient's chest radiographs, we observed catheter's luminal narrowing, that was not present on the initial chest X-ray, in the chest radiograph that was taken 4 months after the insertion of the right subclavian venous port (Fig. 9). It is assumed that the weakened catheter was fractured by the force used during the removal. To find out the exact location of the catheter, pulmonary arteriography was performed (Fig. 10). The patient was referred to an interventional radiologist, and the embolized catheter was successfully removed by the percutaneous approach through the right common femoral artery (Fig. 11).
DISCUSSION
When a subclavian venous catheter is compressed between the clavicle and the first rib, it can cause permanent or intermittent obstruction, and as a result, tearing, transection, and catheter embolization can occur. In 1990, Hinke et al. [3] first described this phenomenon as pinch-off syndrome. Before this, Aitken and Minton [4] named the chest X-ray findings that indicated impending subclavian catheter problems as pinch-off signs. Hinke et al. [3] distinguished pinch-off signs on the following scale when introducing pinch-off syndrome: grade 0, no narrowing in the catheter's course; grade 1, no luminal catheter narrowing, but deviation; grade 2, luminal narrowing as the catheter passes under the clavicle (true pinch-off sign); grade 3, catheter transection between the clavicle and the first rib that is accompanied by embolization of the distal catheter. According to the research by Mirza et al. [5], the most common clinical presentation in patients with pinch-off syndrome was pain with or without swelling at the catheter insertion site, and the next most common was dysfunctional catheter, in other words, problems with blood aspiration or flushing, and the lesser common clinical presentation were accidental discovery of catheter embolization on routine chest X-ray, cardiac palpitation, bilateral chest pain, abdominal pain and nausea, new S3 heart sound, paresis of the ipsilateral arm, etc. The median interval from the time of catheter insertion to pinch-off syndrome was 5.3 months, the average time interval was 5 months, and the longest interval was 60 months from the time of insertion. According to the collective review by Fisher and Ferreyro [6], the rate of serious complications related to embolized catheters including death was 71% in patients who had pinch-off syndrome, and they asserted that the central venous catheter should be removed as soon as possible. Mirza et al. [5] suggested the use of the internal jugular venous route to fundamentally prevent pinch-off syndrome. In fact, the subclavian venous route is being used less frequently because of pinch-off syndrome and other associated complications such as hemothorax, pneumothorax, mediastinal hematoma, vascular perforation, and myocardial injury. However, this practice has some advantages of patient mobility, secured dressing, and rapid and adequate vascular access [7]. A subclavian venous port can be a good choice if an well-trained, experienced faculty is available, especially in the case of totally implantable venous port insertion for chemotherapy because patient comfort is an important consideration in this case. As shown in the aforementioned cases, pinch-off syndrome can occur without any unusual symptoms; therefore, it is necessary to closely observe with repeated chest X-rays of those patients who undergo subclavian venous port insertion; if problems occur with blood aspiration and heparin flushing, the possibility of pinch-off syndrome should be suspected. In the first and second cases, a grade 1 pinch-off sign was observed in the chest radiograph taken immediately after port insertion, and in the third case, pinch-off signs were not observed immediately after port insertion, but grade 2 pinch-off sign was newly observed eventually. Therefore, chest radiographs should be taken after subclavian venous catheterization, and pinch-off signs as well as mechanical complications such as hemothorax and pneumothorax should be checked. In the second and third cases, the authors were unable to predict pinch-off syndrome and only discovered the pinch-off signs by retrospective review. In addition, in the second case, pinch-off syndrome was detected after the venous port was removed, 12 months after the termination of chemotherapy. Therefore, if the venous port is not required, then the catheter should be immediately removed to avoid pinch-off syndrome. Rubenstein et al. [8] and Zieren et al. [9] reported that, while gaining subclavian venous access, cannulation on the lateral side of the mid clavicular line may reduce pinch-off syndrome. Therefore, we conclude that, the basic principles are important for preventing this syndrome. These principles include performing the procedure accurately, observing the patients closely, and removing the venous port immediately, if no longer required.









 XML Download
XML Download