

 ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Granulomatous lobular mastitis (GLM) is a rare inflammatory disease that develops in the breast, and is known to have clinical and imaging characteristics similar to those of breast cancer [1-4]. GLM should be differentially diagnosed from tuberculosis, sarcoidosis, and mycotic and parasitic infections because its histological features include noncaseating granulomas, small abscesses, and inflammation in the lobules [5-7]. The cause of GLM is thought to be an autoimmune reaction to materials secreted from the mammary ducts. In addition, it has been reported that giving birth, breastfeeding, oral contraceptive use and bacterial infections may be relevant factor in the development of GLM [1,8-12]. However, it is still not clearly understood how GLM develops. Therapy includes simple observation, antibiotics, steroid, drainage, excision, and mastectomy, but the optimal treatment is still not determined. It is known that GLM often recurs after treatment [13-15]. Therefore, physicians sometimes find it difficult to choose the right treatment method for patients diagnosed with GLM. The aim of this study is to determine effective treatment methods for GLM as well as to present the author's experience with various treatment methods for GLM.
METHODS
This study involved 50 patients who were diagnosed with GLM and were treated in our institution between January 2005 and December 2009. Their clinical characteristics, treatment processes, and results were analyzed. In all these patients, the lesions were confirmed with a breast examination and imaging evaluation using ultrasonography (US). A definitive diagnosis was made pathologically after a percutaneous US-guided core biopsy was performed. In addition, tuberculosis was ruled out in each patient from the patient's medical history, chest X-ray and polymerase chain reaction test results. The 50 patients were classified into five groups based on the initial treatment methods they underwent, which included observation, antibiotics, steroid, drainage, and surgical excision. The criteria for selecting the method of initial treatment were as follows: patients with mild symptoms or small lesions were observed; patients who were initially thought to have bacterial mastitis underwent antibiotic treatment; patients with multiple lesions or large lesions were treated with steroids; patients with abscess at the time of their diagnosis underwent drainage; and surgical excision was performed on patients who showed mass-forming lesions or localized lesions at the time of their diagnosis. The treatment processes in each group were examined. The recovery period was defined as the time between the initial office visit and the disappearance of the symptoms or the completion of wound healing in the case of surgical treatment. Recurrence was defined as the reappearance of the same symptoms after their initial disappearance or after the surgical removal of the lesion. The patients were followed up in outpatient office visits, and those who recovered and no longer visited the office were followed up via phone interviews.
RESULTS
Clinical features
All the 50 patients were female, with an average age of 37.1 ± 7.9. Thirty-three patients (66%) were in their 30s, and 44 (88%), of childbearing age (below 50). Three patients were breastfeeding at the time of their diagnosis. The main symptoms included a palpable mass in 32 patients (64%), pain in 11 patients (22%), and swelling in 5 patients (10%). Lesions were present in the right breast in 26 patients (52%) and in the left breast in 24 patients (48%). No patient had lesions in both breasts. During the breast examination, 36 patients (72%) were found to have a palpable mass, of which five (10%) had palpable ipsilateral axillary lymph nodes. Nipple retraction was observed in two patients (4%), and fistula was found in one patient (2%). The average size of the measurable lesions was 4.2 ± 2.7 cm. The average follow-up period was 32.0 ± 18.1 months.
Treatment process
Observation
Eight patients underwent observation for their treatment. Five of these eight were found to have mild symptoms with a 1-2 cm sized single lesion or multiple small lesions. The other three patients, whose breast US revealed 3-5 cm sized lesions (tubular lesions that are not localized or lesions with heterogeneous parenchymal echogenicity), chose observation management without other treatment because they were expecting to get pregnant or were breastfeeding. Seven patients improved, but one patient who showed a 5 cm lesion after heterogeneous parenchymal echogenicity had to eventually undergo drainage due to abscess development. There was no case of recurrence during the observation period.
Antibiotic treatment
Three patients underwent antibiotic treatment because they were initially thought to have bacterial mastitis. When their symptoms persisted, they were diagnosed with GLM via a US-guided core biopsy. Among these patients, one gradually improved after having experienced recurrent improvement and worsening of symptoms. Another patient developed an abscess and underwent drainage followed by steroid treatment. This patient eventually recovered after surgical excision due to lesion localization. The other patient, who lives abroad, was not reached for follow-up (Fig. 1).
Steroid treatment
Thirteen patients, most of whom had multiple lesions or large lesions, were treated with steroids. Thirty to 40 mg of prednisolone was orally administered once a day. The dose was lowered to 5 mg when the symptoms improved. Four patients recovered with steroid treatment only (Fig. 2). Another four patients did not respond to the steroid treatment and had to undergo drainage due to abscess development. In one of these patients, the lesion had to be surgically excised because it did not improve even after the drainage. After the surgery, the wound discharge persisted for an extended period. Among the three patients whose condition improved after the drainage, one patient occasionally complained of pain and redness during the observation period. These symptoms were determined to be mild, and the patient was merely observed, without further treatment. Five patients underwent surgical excision because their lesion became localized, with decrease of the lesion size after steroid treatment in two patients; the symptoms persisted or worsened after steroid treatment in two patients; and a side-effect (generalized edema) of the steroid was observed in one patient. All the five patients recovered after the surgery. The patient who experienced a side-effect, however, experienced a relapse after four months.
Drainage treatment
Fourteen patients underwent drainage because abscess had already developed at the time of their diagnosis (Fig. 3). Four patients improved only with drainage treatment, and one patient underwent surgical excision because a localized abscess pocket remained after the drainage treatment. Nine patients additionally underwent steroid treatment because their symptoms persisted after the drainage. Among these patients, three improved, two underwent additional drainage due to persistent abscess, one patient was not available for follow-up, and three patients underwent surgical excision. Among the three patients who underwent surgical excision, one underwent surgical treatment because her symptoms worsened during the steroid treatment, and the other two patients underwent surgical treatment because their lesion became localized during the steroid treatment. After the surgery, one patient showed persistent discharge from a surgical wound and underwent additional steroid treatment. This patient took a long time to recover. There was no sign of recurrence in the three other patients who underwent surgical excision.
Surgical treatment
Surgical excision was performed on 12 patients who showed mass-forming lesions or localized lesions at the time of their diagnosis (Fig. 4). The average size of the lesions was 3.8 ± 2.3 cm. A wide excision method was chosen to remove the GLM lesion and the surrounding normal tissues. After the surgery, all 12 patients recovered without complications, but one patient experienced a relapse after six months and underwent additional surgery, after which no sign of recurrence was observed.
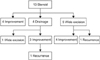
A total of 23 patients underwent surgery, among whom 12 patients underwent surgery as an initial treatment, and 11 patients initially received other treatments and eventually underwent surgery (Fig. 5). Twenty-one of the 23 patients recovered after the surgical excision, but two patients showed signs of recurrence during their observation. In the other two patients who underwent surgical excision after drainage and steroid treatment, wound healing was delayed. Excluding these two patients, the average recovery period was 12.7 ± 9.7 days for 21 patients. In the 12 patients who underwent surgery as an initial treatment, the average recovery period was 11.5 ± 9.2 days.
DISCUSSION
GLM, a rare inflammatory disease that develops in the breasts, was first reported by Kessler and Wolloch [5] in 1972. Its cause and treatment have not yet been clearly identified despite the efforts of many researchers. The treatment methods known to date include observation, antibiotics, steroids, drainage, excision, and mastectomy, but an optimal treatment method still needs to be determined [13-15]. In this study, various treatment methods were applied based on the medical conditions of the patients and on the clinical judgment of the physicians.
It has been reported that GLM is a self-limiting condition and can be expected to disappear on its own within 6-12 months with close surveillance [16,17]. In this study, seven of eight patients improved during their observation. In most of them, the lesions were small and the symptoms were mild; the patient with the larger lesion eventually developed an abscess. Therefore, it is thought that observation management is appropriate only for patients with mild symptoms. Observation management has a disadvantage in that it requires careful follow-up for an extended period, and repeated imaging and histological tests may be needed [18].
Treatment with antibiotics was used for the three patients who had undergone treatment before the diagnosis of GLM was made. The effect of the antibiotic treatment could not be determined in this study because there were so few patients who were given antibiotic study and some of them discontinued their antibiotic treatment after their diagnosis with GLM. In addition, there is no relevant report yet to date on the effect of antibiotic treatment on GLM. Antibiotic treatment of presurgery and postsurgery GLM patients has been attempted, but its effect could not be determined [19]. It is hypothesized that infection could cause GLM, but in this study, no bacterium was detected in the GLM patients. In addition, GLM requires to be distinguished from bacterial infection during its diagnosis, which suggests that antibiotic treatment may not be effective for GLM.
Since DeHertogh et al. [20] first used steroids for GLM treatment, steroid treatment has been tried by many physicians who believe GLM is caused by autoimmune reactions. In this study, 13 patients received steroids as initial treatment, with four of them responding to the treatment and one patient switching treatment methods due to experiencing a side-effect of the steroid. In two patients, the lesions shrunk and became localized. These patients eventually underwent surgical excision. Although steroid treatment was not effective in this study, Hova nessian Larsen et al. [21] reported that 77% of the GLM patients in their study improved with steroid treatment. In addition, many studies have reported the importance and effectiveness of steroids on GLM treatment. The disadvantages of steroid treatment include various clinical outcomes, recurrence with discontinued use of steroids, and potential side-effects such as glucose intolerance or Cushing's syndrome with long-term use of steroids [22].
The drainage method is still controversial in GLM treatment because the incision wound does not heal easily and can leave a fistula tract, and treatment can last for an extended time. Erozgen et al. [23] reported that 14 of the 25 GLM patients developed abscess and underwent drainage followed by steroid treatment, and suggested that drainage is the first choice of treatment for patients who develop an abscess. In this study, 14 patients underwent drainage due to abscess formation around the GLM lesions. Among them, four patients recovered with drainage only without any wound-related issues, but their recovery took a long time. In the other nine patients, the lesions persisted after the drainage, and these patients underwent additional steroid treatment. Three of these nine patients recovered with steroid treatment, but the other six patients had to undergo repetitive drainage or surgical excision due to persistence of their symptoms. Abscess must be treated by drainage, but it is suggested that the drainage be followed by additional appropriate therapies.
Surgical excision was considered a critical treatment method for GLM when GLM was first reported in the 1970s [8]. It was later suggested, however, that GLM should not be treated surgically to avoid complications such as fistula formation and poor wound healing. In addition, a higher recurrence rate was reported after surgical excision compared to the recurrence rate after steroid treatment. Therefore, steroids became a popular means of GLM treatment [5,22,24-26]. Recently, however, attention is being given again to surgical treatment, with studies on this method continuing. In this study, a wide excision method was used to remove the GLM lesion and the surrounding normal tissues in patients who had a mass or localized lesion at the time of the diagnosis. In addition, selected patients, including those whose lesions became localized and resectable after they underwent other kinds of treatment, and patients who did not respond to other treatment modalities, were treated via surgical excision. All the 12 patients who underwent surgical excision as an initial treatment recovered faster, with an average recovery period of 11.5 ± 9.2 days compared to the recovery periods for the other treatment methods (data not shown). The advantages of surgical excision include fast recovery and more accurate diagnosis of a GLM that appears similar to breast cancer.
Among the 23 patients who underwent surgical excision, 11 patients initially underwent other types of treatment. Two of these 11 patients experienced delayed wound healing after surgical excision. One patient initially underwent steroid treatment followed by drainage due to abscess formation, and eventually underwent surgical excision. The other patient initially underwent drainage followed by additional steroid treatment, and was eventually treated via surgical excision because her lesion became localized during the steroid treatment. Some studies have reported that the lesions persisted or that GLM recurred when the excision was incomplete. It is thought that the delayed wound healing and recurrence that were observed in this study might have occurred for the same reason [3,17,21,27]. A lesion that does not respond to other kinds of treatment tends to be diffuse in distribution without a clear boundary separating it from normal tissue. It might not be possible for surgery to completely remove such lesions. To ensure the success of surgical treatment, the surrounding normal tissue, the affected breast skin, the fistula, and the sinus track should be completely removed even if the lesions become localized and resectable.
In this study, two of the 23 patients who underwent surgical excision experienced a relapse. One patient was 35 years old and had a relatively large lesion distributed from the upper center to the mid-outer left breast at the time of her diagnosis. The lesion of this patient was mass-forming, and it was removed via surgery. Six months after the surgery, an additional excision was made because a 1-cm abscess pocket was detected during the US. The other patient, who was 42 years old, underwent surgical excision because her symptoms worsened during the steroid treatment and a side-effect (generalized edema) of the steroids occurred. During the initial US, the lesion in the upper inner quadrant of the patient's left breast was observed to have diffusely extended to the periphery. The patient recovered without complications after the surgery, but her symptoms reappeared in the surgery site after four months. In this study, the recurrence rate after surgical excision was 8.7%, which is a favorable outcome compared to the recurrence rates of 6-21% reported in other studies [3,15,19].
In conclusion, the optimal treatment for GLM has still not been determined because the clinical course of GLM is complex and the outcome of each treatment modality is variable. Therefore, a proper treatment method should be chosen on a case-by-case basis. Among the treatment methods, surgical excision showed particularly fast recovery and a high success rate. We think surgery may play an important role when a lesion is determined to be mass-forming or appears localized as an abscess pocket during breast examination or imaging study. In surgical excision, the surrounding normal tissue as well as the affected tissue should be removed.




 XML Download
XML Download