

 ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The prevalence of peripheral arterial diseases has been increasing along with the increase of aged populations in most developed countries [1]. The same phenomenon is found in Korea along with the necessity for invasive treatment for diseases. Recent advances in endovascular treatment techniques and tools are rapidly changing the range of indications within peripheral arterial diseases as well as treatment plans for these diseases [2]. Such changes in treatment schemes are reflected in TASC II (2007), which reports the lesions that are mostly in the domain of surgical treatment and that can now be treated by endovascular means with similar results [3]. As generally recognized, endovascular treatment is an invasive means of treatment but is less invasive than surgical means. And it can be applied to patients with relatively high risks against invasive treatment, which suggests a wider range of the indicants of invasive treatments [1,4].
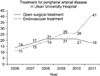
The number of invasive treatment cases of patients with peripheral arterial disease was also increased in Ulsan University Hospital. Such increase is mostly due to the growing number of endovascular treatment cases. The proportion of surgical treatment, however, was not decreased but maintained at a constant level (Fig. 1). We designed this study for two purposes: first, to investigate the trends of surgical treatment while the role of endovascular treatment expanded and surgical treatment still played a role under this changing circumstance; secondly, to analyze the trends of surgical treatment at a single, mid-sized medical institution.
METHODS
Materials
We investigated the retrospectively collected records of peripheral arterial disease patients who had received treatment at a single hospital during the period from March 2006 to December 2011. With every case, treatment plans were determined by the in-house vascular meetings with two vascular surgeons and one radiologist. Preoperative clinical characteristics and postoperative results and complications were analyzed based on the medical records of all the patients. In order to determine the trends of surgical treatment, we investigated the number of surgical treatment cases and endovascular treatment cases over the entire study period and divided the cases into two groups under the treatment time period, one is the "surgical period" group for the cases before 2009 when surgical treatment showed higher frequencies and the other the "endovascular period" group for the cases from 2009 onward when endovascular treatment was more frequent (Fig. 1).
Disease categories
The study cases were classified into acute ischemia and chronic ischemia lesions based on the urgency of the onset of the symptom. And, the urgency was determined from clinical characteristics of the symptoms rather than the generally applied time factor. Further categorization of each type of lesion was made based on the method proposed by Rutherford as follows:
Categories of acute limb ischemia lesion: according to the Rutherford classification, these cases were divided into the categories of viable, threatened, and irreversible limb, which were denoted with letters I, II and III, respectively
Categories of chronic limb ischemia lesions: according to the Rutherford classification, these cases were divided into the categories of mild claudication, moderate claudication, severe claudication, ischemic resting pain, minor tissue loss and major tissue loss, which were denoted with numbers 1, 2, 3, 4, 5, and 6, respectively [3].
Classification of surgical treatments
Classification by location of surgery
Depending on the location of the vascular lesion that required exposure during surgery, the cases were divided into those above inguinal ligament (suprainguinal, SI), below inguinal ligament to above knee (thigh, T) and below knee (BK). When two or more locations were involved, the cases were recorded as "T" when the lesions were limited in between the inguinal ligament and the knee, "SI" when it included the area above the inguinal ligament and "BK" when it included the area below the knee.
Classification by surgical method used
The case was classified as a 'bypass' when bypass procedure was performed by creating vascular exposures at two or more locations regardless of the conduit types, a 'nonbypass operation' (NBO) when thrombectomy, embolectomy, endarterectomy or patch angioplasty was performed with only one point vascular exposure, or 'hybrid' when both surgical treatment and endovascular treatment were performed.
Result definitions
The result of surgery was defined as a 'technical success' when the desired reperfusion was successfully accomplished by surgery as anticipated, a 'functional success' when ankle-brachial index (ABI) increased by 0.2 compared with the preoperative level or when the tissues of the lesion at the location where recovery had been anticipated before surgery actually revived. 'Patency' was defined for the cases where blood flow was radiologically confirmed or when ABI did not decrease by more than 0.1 compared with the prechecked level. For the analysis of complications, occurrences of pneumonia within one month after the surgery, new or deteriorated renal failure, hemorrhage that required surgical intervention, infection of operation site, myocardial infarction and cerebral stroke were investigated.
Statistical analysis
Tests of statistical significance comparing were conducted using χ2 and Fisher exact test for categoric variables, and t test for continuous variables. A probability value of P < 0.05 was considered statistically significant. All statistical analyses and drawing graphs were performed using SPSS ver. 11.0 (SPSS Inc., Chicago, IL, USA) and R package (ver. 2.15).
RESULTS
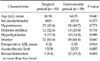
A total of 112 cases were included in this study. The mean age of patients was 65.9 years (range, 15 to 93 years) and male:female ratio was 89:23. The number of cases where patients had accompanying major risk factors for arteriosclerosis such as hypertension, diabetes mellitus, hyperlipidemia and smoking habit was 47 (42.0%), 27 (24.1%), 19 (17.0%) and 60 (62.0%), respectively. The mean estimated glomerular filtration rate (eGFR) calculated based on age, gender and creatinine level was 70.98 mL/min and the number of cases with eGFR below 50 was 13 (11.6%). The number of acute ischemia and chronic ischemia cases was 47 and 65, respectively (Table 1).
Classification of the cases into treatment time period groups showed 53 cases treated during surgical period and 59 cases during endovascular period. Mean age of patient in each period group was 66.96 and 64.95, respectively, and male:female ratio was 44:9 and 45:14, respectively. The number of patients with hypertension, diabetes mellitus, hyperlipidemia and smoking habit was 23 (43.4%), 12 (22.6%), 9 (17.0%) and 32 (60.4%), respectively, in surgical period group and 24 (40.7%), 15 (25.4%), 10 (16.9%) and 38 (64.4%), respectively in endovascular period group (Table 2).
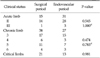
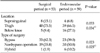
The preoperative average ABI for each period was 0.32 and 0.33, respectively. The ratio of acute versus chronic lesions was 15:38 for surgical period and 32:27 for endovascular period. The number of cases in which revascularization was required at two or more locations using an invasive method including surgery was 5 (9.4%) during surgical period and 22 (37.3%) during endovascular period (Table 2). Preoperative categorization of the lesion type for each period group resulted in findings of category I and II of acute ischemia lesions in 14 and 1 cases respectively in surgical period group and 28 and 3 cases respectively in endovascular period group. Category 3, 4, 5 and 6 of chronic type lesions were found in 17, 6, 11 and 4 cases respectively in surgical period and 15, 3,l 7, 3 cases in endovascular period. Separate categorization of critical limb type consisting of categories 4, 5 and 6 resulted in finding of 21 such cases in surgical period and 14 cases in endovascular period (Table 3). Classification by the location of surgery revealed 8, 40 and 5 cases respectively of SI, T and BK category in surgical period and 4, 39 and 16 cases in endovascular period. When classified by the method of surgery used, the number of cases of bypass, NBO and hybrid was 33, 19 and 1 during surgical period and 23, 30 and 6 during endovascular period (Table 4).
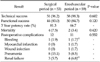
Technical success rate in surgical period group and endovascular period group was 96.2% (51/53) and 98.3% (58/59), and functional success rate was 83.0% (44/53) and 84.7% (50/59), respectively. Three-year patency rates were 81.3% and 66.7% respectively. Mortality cases were 4 in surgical period and 2 in endovascular period. Postoperative complications were one bleeding, 8 pneumonias, and 3 renal failures in surgical period, and one myocardial infarction, one wound infection, 5 pneumonias, 3 renal failures and one bleeding with renal failure case in endovascular period (Table 5). Death within one month from surgery occurred in 4 cases (7.5%) in surgical period and 2 cases (3.39%) in endovascular period and the occurrences of complications were observed in 12 cases (22.6%) in surgical period and 11 cases (18.6%) in endovascular period (Table 5).
Subgroup analysis of BK surgeries performed during endovascular period showed 11 acute cases and 5 chronic cases, showing more acute cases compared with 3 cases and 2 cases respectively during surgical period. Classification by surgical method used revealed 6, 10 and 0 cases respectively of bypass, NBO and hybrid during endovascular period compared with 2, 3 and 0 cases respectively during surgical period, indicating increased use of NBO (Table 6).
Hybrid procedure was performed in 1 case in surgical period but the number increased to 6 in endovascular period. Summary of 6 cases in which hybrid procedure was performed during endovascular period is shown in Table 7.
DISCUSSION
The treatment of peripheral arterial disease is continuously changing along with the advancement of endovascular techniques. Influenced by such changes, the lesions which could only be treated with surgical methods can now be handled with endovascular methods [5]. In addition to treatment method, changes also occurred in the inclusion of subjects for endovascular treatment as evidenced by the fact that patients with higher risks are now indicated with this method and more cases than just critical limb ischemia cases, including those aimed at improving quality of life, are now included as the subject of invasive treatment [6].
The number of surgical treatment cases in this study was not significantly changed in both surgical period and endovascular period. Considering that surgical period was shorter than endovascular period by two months, the 6-case difference between the period groups is ignorable and, therefore, it can be said that there was no actual difference in the number of cases between the two periods. The reason for an increase of peripheral arterial disease cases that required invasive treatment was an increased number of endovascular treatment cases in our hospital (Fig. 1). It may be due to an extension of indication for endovascular treatment (data not shown). Considering the facts that there has been no change in the number of surgical treatment cases in age, gender and preoperative conditions of patients, such increase does not mean there have been an increased number of patients with high risks. Such development shows clear distinction from the previous phenomenon in which the advancement of endovascular aneurysm repair techniques resulted in the application of surgical treatment to patients with abdominal aortic aneurysm with higher risks than was previously possible [7]. The degree of risk in the cases included in surgical treatment did not show any increase nor was there any significant difference of postoperative rates of complications and mortality. However, the number of acute cases increased considerably during endovascular period compared with the previous period. This contrasts with the fact that the number of acute cases that received endovascular treatment did not increase, which may be because acute embolism, which is the main cause of acute limb ischemia, can be treated more effectively with surgical means than endovascular methods [6,8]. Also, it may be partly because it takes longer to mobilize the endovascular surgery team and equipment leaving the readily available surgical treatment as an inevitable option in an emergency situation such as the onset of acute limb ischemia.
Surgical treatment has higher risks since suprainguinal approach requires general anesthesia and abdominal incision. In the cases of below knee approach, in particular, surgery tends to be performed in noncritical cases and with more care because postoperative patency rate is lower than that of distal approach [9]. According to the records in Ulsan University Hospital, the number of the cases of suprainguinal approach in endovascular period decreased to half compared with the previous period (Table 4). It may reflect a new trend of applying an endovascular method, if possible, to suprainguinal lesions that have high operational risk. The number of BK lesion cases increased considerably compared with previous period, because most of the cases were of acute limb ischemia (Table 6). The number of surgical treatments of BK lesions in chronic limb ischemia cases was 2 cases in surgical period and 5 cases in endovascular period showing no significant increase; The number of bypass surgery also was 2 cases and 6 cases respectively, showing not much increase compared with NBO cases. The roles of endovascular treatment and surgical treatment can be deduced more clearly from the results of hybrid procedures performed during endovascular period. In 6 cases of this period in which hybrid procedure was performed, surgical repair was mostly limited within the thigh, while suprainguinal lesions and BK lesions were resolved by endovascular method (Table 7).
The advancement of new treatment techniques also allows the existing treatment methods to evolve to more safe ones [10]. The advancement of endovascular treatment method for peripheral arterial disease has continuously been improved toward substituting existing surgical methods [11]. Such advancement of endovascular treatment methods seems to have increased the applicable range of invasive treatment in peripheral arterial disease in general. It may be partly because of the fact that suprainguinal lesions can now be treated with endovascular methods, thereby making it possible for the patients with higher risks than was previously possible to be included in the indicants of these methods. Thanks to these advanced endovascular methods, the overall number of invasive treatment of patients with peripheral arterial disease with limb ischemia increased in our hospital. While the total number of such cases increased, the number of surgical treatments for chronic limb ischemia decreased, which may be because some of them were replaced by endovascular treatment. However, the number of surgical treatments for acute limb ischemia increased.
In conclusion, surgical treatment seems to be a complementary method to endovascular treatment for chronic limb ischemia but still seems to play a major role for acute limb ischemia.



 XML Download
XML Download