

 ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The survival of gastric cancer has steadily improved in the past decade along with advanced diagnostics and screening programs and improvement of chemotherapy. However, the prognosis of unresectable gastric cancer is still poor, with peritoneal seeding, distant metastasis, and distant lymph node metastasis.
Para-aortic lymph node (PAN) metastasis is considered a distant lymph node metastasis. The prognosis of gastric cancer with PAN metastasis is quite poor even after prophylactic para-aortic lymphadenectomy [1]. For this reason, systemic chemotherapy is commonly preferred as a primary mode of treatment in these patients. Various kinds of chemotherapeutic regiments including 5-fluorouracil, cisplatin, irinotecan, taxans, and capecitabine were widely used in the past decades. The clinical response ratio of palliative chemotherapy in gastric cancer with PAN metastasis was reported up to 68.8% [2]. Recently several cases of therapeutic gastrectomy with para-aortic lymphadenectomy after chemotherapy were reported [2-4], but the efficacy of gastrectomy with para-aortic lymphadenectomy after chemotherapy remains still unclear.
Laparoscopy-assisted gastrectomy is an option in the treatment of gastric cancer, and the indication for this procedure has extended to locally advanced gastric cancer. However, there was no report of laparoscopic para-aortic lymphadenectomy in gastric cancer except laparoscopic biopsy of PAN for the staging [5]. Herein, we report three cases of laparoscopy-assisted gastrectomy with para-aortic lymphadenectomy after palliative chemotherapy for far advanced gastric cancer for the first time in Korea.
CASE REPORTS
The details of three cases are summarized in Table 1.
Case 1
A 45 year-old man was diagnosed with a poorly differentiated adenocarcinoma in the gastric angle by gastroscopy. A positron emission tomography-computed tomography (PET-CT) suggested left para-aortic and aortocaval lymph node metastasis. After completing 4 cycles of XELOX, the patient showed partial response to the chemotherapy with decreased extent of primary cancer and retroperitoneal lymph nodes. After the confirmation of no evidence of seeding in the diagnostic laparoscopy, he underwent a successful laparoscopic extended total gastrectomy with para-aortic lymphadenectomy with the usual 5-port system without additional port insertion. The total operative time was 370 minutes and para-aortic lymphadenectomy took 100 minutes. The estimated blood loss (EBL) was 125 mL. The pathologic results revealed no residual primary tumor and no lymph node metastasis in harvested 77 lymph nodes (LNs; 16a2 [0/3], 16b1 [0/5]). He recovered and was discharged at postoperative 8 days without any complications.
Case 2
A 46 year-old woman was diagnosed with a poorly differentiated adenocarcinoma in the gastric body, and CT suggested bulky perigastric lymph nodes (station 3 and 7, 2.0 cm and 1.0 cm) and left PAN metastasis (2.2 cm). After completing 4 cycles of XP, she showed partial response to the chemotherapy with decreased sizes of perigastric (0.9 cm and 0.6 cm) and left PANs (0.8 cm). She underwent laparoscopic subtotal gastrectomy with para-aortic lymphadenectomy, but the small branch of the left renal vein was injured at the end of para-aortic lymphadenectomy, so bleeding control was performed via minilaparotomy. The total operative time was 415 minutes and para-aortic lymphadenectomy took 97 minutes. The EBL was 200 mL. The pathologic results revealed submucosa tumor and 6 LNs metastases in 58 harvested LNs (16a2 [0/0], 16b1 [0/11]). She was discharged at 11 days postoperatively after conservative management due to a large amount of ascites.
Case 3
A 63 year-old man was diagnosed with a poorly cohesive adenocarcinoma in the gastric lower body, and a PET-CT suggested multiple perigastric and left PAN metastases. After completing 7 cycles of XP and 5 cycles of Xeloda, he showed a partial response to the chemotherapy with decreased sizes of perigastric and left PANs. He underwent laparoscopic subtotal gastrectomy with para-aortic lymphadenectomy successfully. The total operative time was 310 minutes and para-aortic lymphadenectomy was performed during 93 minutes. The EBL was 150 mL. The pathologic results revealed subserosa tumor and 3 LNs metastases in harvested 35 LNs (16a2 [0/0], 16b1 [0/8]). He was discharged at 8 days postoperatively without any complications.
Laparoscopic para-aortic lymphadenectomy
All laparoscopic para-aortic lymphadenectomies were performed with the standard 5-port system used in laparoscopy-assisted total gastrectomy without any additional port insertion (Fig. 1). An ultrasonic cutting device (SonoSurg, Olympus, Tokyo, Japan) and LigaSure (Valleylab, Boulder, CO, USA) was used to minimize postoperative bleeding and ascites after lymphadenectomy.
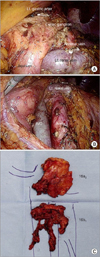
After laparoscopy-assisted subtotal or total gastrectomy with complete omentectomy and D2 lymphadenectomy, PAN dissection proceeded from 16b1 area to 16a2 area. The infra-pancreas mesocolon was first dissected to enter the retroperitoneal space. After exposure of Gerota's fascia of left kidney, splenic flexure was mobilized to take down transverse colon and mesocolon toward the lower abdomen. Following identification of the left renal vein (superior border), left gonadal vein (left side border), Treitz ligament (right side border), and inferior mesenteric artery (IMA) (inferior border), 16b1 PAN including lateroaortic, preaortic, and interaortocaval area were dissected from IMA to left renal vein. For 16a2 lymph node dissection, the pancreas was mobilized from retroperitoneum. The supra-left renal area was dissected first, and the dissection proceeded up to celiac ganglion. The completed para-aortic lymphadenectomy and specimen are shown in Fig. 2.
Bowel reconstruction such as uncut Roux en Y G-J stomy and Roux en Y E-J stomy was performed after surgical hemostasis and irrigation of para-aortic lymphadenectomy area.
DISCUSSION
In advanced gastric cancer, the prevalence of microscopic metastases in the para-aortic region is 10% to 30% [6,7]. Because the 5-year overall survival rate of patients with PAN metastases is less than 20% even after prophylactic dissection, D2 lymphadenectomy plus PAN dissection is not recommended in curable gastric cancer [1]. PAN involvement is now considered M1 in tumor-node-metastasis (TNM) classification system (7th edition) as reported by the American Joint Committee on Cancer.
In unresectable gastric cancer, the isolated PAN metastasis seems to be different from other metastasis. Park et al. [8] reported that PAN-only metastasis showed better survival and longer time to other organ metastasis compared with single or multiple organ metastases, and Oyama et al. [2] reported high clinical response ratio of preoperative chemotherapy in gastric cancer with pathologically positive PAN. However, the clinical characteristics of isolated PAN metastasis have not been comprehensively described.
As various chemotherapeutic agents and regimens have been developed, several studies reported that short-term outcome of curative gastrectomy after neoadjuvant chemotherapy in unresectable gastric cancer including PAN metastasis. Sym et al. [9] reported that R0 resection was possible in 71% after neoadjuvant chemotherapy with docetaxel, cisplatin and capecitabine. Oyama et al. [2] reported that combination preoperative chemotherapy with docetaxel, cisplatin, and S-1 and gastrectomy with PAN dissection was extremely effective and feasible for advanced gastric cancer with PAN metastasis, and reported 2-year overall survival at 93.8%. However, a consensus of neoadjuvant chemotherapeutic regimen was not established and there were few prospective studies in gastric cancer with PAN metastasis. Therefore, the efficacy of gastrectomy with PAN lymphadenectomy after palliative chemotherapy remains unclear, especially for advanced gastric cancer with isolated PAN metastasis.
In the present cases, all patients had isolated PAN metastasis and showed partial response to capecitabine-based chemotherapy. In case 2, preoperative advanced gastric cancer was changed to early cancer after chemotherapy, and even in case 1, the pathologic result showed complete regression. Furthermore there was no metastasis of PAN in the final pathologic results, so we could achieve R0 resection in all cases and TNM stages of the patients migrated to lower stages eventually compared with preoperative stage. However, it seems premature to predict their prognosis according to postoperative stage. Long-term follow-up will be needed to evaluate whether this downstaging effect could influence the actual survival or not.
Most importantly, the present case series report is the first report of laparoscopic para-aortic lymphadenectomy in Korea. Laparoscopic surgery is a well-established minimally invasive surgical alternative to open surgery and has advantages of reduced postoperative pain, shorter hospital stays, and less complications [10]. Despite its advantages, laparoscopic para-aortic lymphadenectomy have not been reported because of its technical difficulty. The present cases report showed that laparoscopic para-aortic lymphadenectomy could be performed without additional port insertion, and that the mean operation time and mean EBL were acceptable compared with open surgery. Considering the number of retrieved lymph nodes in para-aortic region, laparoscopic para-aortic lymphadenectomy was feasible oncologically. It was also significant that all patients were recovered and discharged without any significant complications.
There was 1 case of intraoperative bleeding due to injury of small branch of left renal vein during 16b1 area dissection. The left renal vein was clamped with two endo bulldogs under laparoscopic view before laparotomy, so it was possible to prevent massive bleeding and to control the bleeding via minilaparotomy.
In conclusion, laparoscopic para-aortic lymphadenectomy in gastric cancer was feasible in terms of technique. However a multi-institutional clinical phase II study is needed to quantify the short-term benefit and long-term oncologic outcome of laparoscopy-assisted gastrectomy with para-aortic lymphadenectomy after chemotherapy for advanced gastric cancer with isolated PAN metastasis.


 XML Download
XML Download