

 ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Peritoneum is one of the most frequent sites of metastasis in pancreatic cancer [1]. However, it is difficult to detect microscopic disease spread in the peritoneum during the operation unless it forms visible lesions in the peritoneum. Peritoneal cytology has been used as clinical parameters for prognostication of gastric [2] or gynecologic malignancies [3]. However, the role and prognostic relevance of peritoneal cytology for pancreatic cancer have not been well defined. Some have reported positive peritoneal cytology as a poor prognostic factor of pancreatic cancer [4,5], but others have regarded positive cytology without any other evidence of distant metastasis not as an independent prognostic factor for overall survival of pancreatic cancer [6-8].
Moreover, there has been limited number of studies dealing with postoperative peritoneal drainage fluid for the evaluation of free cancer cells in pancreatic cancer. To detect minimal residual disease after R0 resection, peritoneal drainage fluid can be used as an important material for the evaluation of free cancer cells in the peritoneum.
Furthermore, detection methods for peritoneal micrometastasis are another challenge. Most of the previous studies have used Papanicolaou's method for the detection of free cancer cells in peritoneal fluids [4-10]. However, conventional cytologic examination has limited sensitivity for detecting peritoneal micrometastasis, and it can have biased results according to pathologists. A recent study reported increased sensitivity of cytologic examination using reverse transcription-polymerase chain reaction for the peritoneal fluid of pancreatic cancer patients [11], or using fluorescent in situ hybridization (FISH) for brush cytologic examination for patients with malignant biliary obstruction [12] and pancreatic cancer [13].
In this study, the authors investigated the prognostic relevance of cytologic examination of peritoneal washing and postoperative peritoneal drainage fluid using the FISH technique in potentially resectable pancreatic cancer patients.
METHODS
From 2005 to 2006, patients with potentially resectable pancreatic adenocarcinoma undergoing pancreatectomy were prospectively enrolled. The demographic and pathologic characteristics of the patients including follow-up data on recurrence, FISH examination for p53 deletion in peritoneal washing fluid and peritoneal drainage fluid were prospectively collected.
Peritoneal washing fluid and peritoneal drainage fluid were collected according to the following protocol. At the beginning of the operation, peritoneal lavage with 1 L of normal saline was performed and the lavage fluid was collected in a sterile bottle mixed with same amount of Saccamano's cytology fixative. At the end of the operation, 3 Silastic peritoneal drainage tubes were placed at the operation field. At postoperative day 2, 100 mL of peritoneal drainage fluid was collected in the same amount of Saccamano's cytology fixative. For conventional cytologic examination, after centrifugation of the collected fluid for 3 minutes at 2,000 rpm, direct smears were prepared and fixed in 95% ethanol and were stained with Papanicolaou's method. All slides were reviewed by an experienced cytopathologist.
FISH examination was performed as follows. After centrifugation of the collected fluid for 5 minutes at 1,000 rpm, the supernatant was removed and the pellet was resuspended with 1 × phosphate buffered saline. The suspension was centrifuged for 5 minutes at 1,000 rpm, and after removal of the supernatant, 5 mL of 0.075 M KCl was added. After incubation for 25 minutes in a 37℃ water bath, 1 mL of Carnoy fixative was added. The suspension was centrifuged for 5 minutes at 1,000 rpm and the supernatant was removed. The pellet was resuspended with 5 mL of Carnoy fixative and direct smears were prepared at a cellular density of 1 × 106/mL. A dried slide was incubated with 50 mL of 0.1% NP-40/2×SSC for 30 minutes in a 37℃ water bath and dehydrated with 70%, 85%, and 100% ethanol for 3 minutes each. Under protection from light, a FISH probe (LSI p53 [17p13.1] SpectrumOrange probe; Vysis Inc., Downers Grove, IL, USA) was hybridized with the prepared slide. After 3 minutes of denaturation at 75℃, the slide was incubated for 24 hours at 39℃. After hybridization, the slide was incubated two times with 50% formamide/2×SSC for 10 minutes at 46℃, 2×SSC for 10 minutes at 46℃, and 0.1% NP-40/2×SSC for 5 minutes at 46℃. For counterstaining, 10ul of DAPI was added to the slide. With a cutoff value of 10%, the slide was examined with a fluorescent microscope.
RESULTS
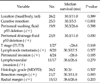
The demographic findings of the study subjects are listed in Table 1. The mean age of the study subjects was 60.1 years and the male to female ratio was 2.5 to 1. Surgery with curative intent was performed in 25 patients (89.3%). None of the patients had malignant cells detected with Papanicolaou's method. The detection rates for p53 deletion in the peritoneal washing fluid and peritoneal drainage fluid were 32.1% (n = 9, Fig. 1) and 17.9% (n = 5), respectively. p53 deletion was not detected in any of the peritoneal washing or peritoneal drainage fluids in 13 patients (46.4%), and p53 deletion was detected in both the peritoneal washing and peritoneal drainage fluid in 1 patient (3.6%). Twenty-three patients (82.1%) received adjuvant treatment. Fourteen patients (77.8%) had concurrent chemoradiation therapy followed by gemcitabine based maintenance chemotherapy. One patient (5.6%) had radiation therapy only, and 5 patients (27.8%) had gemcitabine based chemotherapy only. All of the patients were followed up for survival analysis for at least 5 years. Twenty-three patients (82.1%) died during the follow-up period, and 25 patients (89.3%) experienced recurrence. The pathologic characteristics of the patients are presented in Table 2. Lymph node metastasis was identified in 20 patients (71.4%) and 7 patients (25.0%) had microscopic positive resection margin.
Tumor characteristics according to p53 deletion
Nine patients (32.1%) had p53 deletion detected in the peritoneal washing fluid. Patients with p53 deletion detected in the peritoneal washing fluid had comparable T stage (T3, 9/9 vs. 18/19, P = 1.000), lymph node metastasis (6/9 vs. 14/19, P = 1.000), perineural invasion (9/9 vs. 15/19, P = 0.273), and lymphovascular invasion (6/9 vs. 11/19, P = 0.937) compared with those without p53 deletion. Patients with p53 deletion detected in the peritoneal washing fluid had comparable radial margin positive rate (4/9 vs. 4/19, P = 0.405) or recurrence rate (8/9 vs. 17/19, P = 1.000) between those with or without p53 deletion detected in the peritoneal washing fluid.
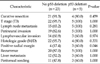
Five patients (17.9%) had p53 deletion detected in the peritoneal drainage fluid (Table 3). Patients with p53 deletion detected in the peritoneal fluid had positive radial margin more frequently (3/5 vs. 4/23, P = 0.046). The overall recurrence rate was comparable between those with or without p53 deletion detected in the peritoneal drainage fluid (5/5 vs. 20/23, P = 0.284).
Eight patients had p53 deletion in the peritoneal washing fluid only. Comparing these patients with 5 patients who had p53 deletion detected in the peritoneal drainage fluid, T3 stage (100% vs. 100%, P = 0.110), lymph node metastasis rate (62.5% vs. 100%, P = 0.376), perineuralinvasion rate (100% vs. 100%, P = 0.110), lymphovascular invasion rate (62.5% vs. 60.0%, P = 0.620) were comparable between two groups. Radial resection margin positive rate was higher in patients with p53 deletion in peritoneal fluid than those with p53 deletion in peritoneal washing fluid only (100% vs. 25.0%, P = 0.039).
Survival outcome according to p53 deletion
Overall median survival of the study subjects was 17.8 months (95% confidence interval, 13.8 to 21.8). According to peritoneal washing fluid analysis, overall survival (3-year survival rate, 33.3% vs. 21.1%; P = 0.961), disease free survival (3-year disease free survival rate, 11.1% vs. 10.5%; P = 0.742), time to local recurrence (median, 17.7 vs. not reached; P = 0.657), time to liver metastasis (median, 11.4 vs. not reached; P = 0.343), and time to peritoneal metastasis (median, 26.6 months vs. 30.3 months, P = 0.598) were comparable between those with or without p53 deletion.
According to the peritoneal drainage fluid analysis, overall survival (3-year survival rate, 0% vs. 30.4%; P = 0.223), disease free survival (3-year disease free survival rate, 0% vs. 13.0%; P = 0.277), time to local recurrence (median, 11.0 months vs. 53.6 months; P = 0.198), and time to liver metastasis (median, 11.4 months vs. 18.8 months; P = 0.797) were comparable between those with or without p53 deletion, but time to peritoneal metastasis was shorter in patients with p53 deletion than in those without p53 deletion (median, 11.1 months vs. 30.3 months; P = 0.030) (Fig. 2).
Prognostic factors for disease free survival of resectable pancreas cancer
Disease free survival of resectable pancreas cancer was associated with surgery with curative intent (P = 0.015) or lymphovascular invasion (P = 0.058). Peritoneal metastasis free survival was associated with surgery with curative intent (P < 0.001), p53 deletion detected in peritoneal drainage fluid (P = 0.030), and positive resection margin (P = 0.093) (Table 4). From the multivariate analysis, palliative resection and p53 deletion detected in the peritoneal drainage fluid were independent factors for peritoneal metastasis free survival (Table 5).
DISCUSSION
Most pancreatic cancers have cytogenetic alterations. Human pancreatic cancers usually have an increased copy number of c-myc, a decreased copy number of p16, deletion of p53, loss of chromosome 18q and gain of chromosome 20q [13]. Our previous study showed that all of the pancreatic cancer tissues had p53 deletions detected by the FISH technique [13]. As a consequence, the authors selected p53 deletion as a cancer cell detection marker in peritoneal washing and peritoneal drainage fluid.
The clinical impact of peritoneal cytology for pancreatic cancer is under debate. Poor survival outcomes in patients with positive peritoneal cytology have been suggested [7,11] but some have reported that positive peritoneal cytology alone does not contraindicate radical surgery in patients with resectable pancreatic cancer [6,8,14,15]. Moreover, positive cytology is not a contraindication of curative surgery for colon cancer [16] or gynecological cancers [17]. In this study, there were no patients with positive cytology using conventional cytologic examinations. Peritoneal washing fluid analysis with the FISH technique was not related with overall or disease free survival and local or systemic recurrence. However, peritoneal drainage fluid analysis with the FISH technique was related with early peritoneal metastasis; therefore, microscopic residual disease detected with the FISH technique may have had an important role in the prognosis of cases with resectable pancreatic cancer which did not have visible metastasis at the time of the operation. Previously, postoperative cytology for lung cancer [18] or esophageal cancer resection [19] showed increased recurrence and shorter survival based on a higher incidence of distant metastasis. In pancreatic cancer, Ishikawa et al. [20] first reported the prognostic relevance of drain cytology for pancreatic cancer which revealed local recurrence was more frequent in patients with positive drain cytology. However, in this study, neither the rate of local recurrence nor the time to local recurrence was affected by p53 deletion detected in peritoneal drainage fluid. Instead, p53 deletion detected in peritoneal drainage fluid was associated with early peritoneal metastasis. Pancreatic cancers usually infiltrate into retroperitoneal nerve plexuses [21] or lymphatic tissues [22] on a microscopic level although macroscopic tumors are confined to the pancreas. The data of this study suggest that microscopic residual disease that outflows from the vessels and lymphatics at the operation bed flows into the peritoneal cavity, which results in peritoneal metastasis. Moreover, since the survival of pancreatic cancer patients is dependent on distant metastasis rather than local recurrence, prediction of peritoneal metastasis has more prognostic relevance than local recurrence.
Traditionally, the prognostic value of the cytologic examination of peritoneal washing fluid in pancreatic cancer has been evaluated by Papanicolaou's method. The detection rate of malignant cells in peritoneal washings from potentially resectable pancreatic cancer using Papanicolaou's method has been reported to range from 5% to 32% [4-10]. In this study, none of the patients with resectable pancreatic adenocarcinoma had positive cytology for both peritoneal washing and peritoneal drainage fluid. Because this study included higher portion of patients who underwent curative resection, positive cytology rate would be lower than other reports. Moreover, limitation in study subject number would have reduced positive cytology rate. On the other hand, p53 deletion was detected with the FISH technique in 32.1% of the peritoneal washing fluids and 17.9% of the peritoneal drainage fluids. p53 deletion detected in the peritoneal washing fluid was not associated with tumor stage or recurrence. However, p53 deletion detected in peritoneal drainage fluid was associated with positive radial margin which reflects the presence of microscopic residual disease. Moreover, p53 deletion detected in peritoneal drainage fluid was associated with early peritoneal metastasis. Therefore, the low sensitivity of the conventional cytologic examination can be overcome with the FISH technique which can identify microscopic residual disease which can predict early recurrence.
In conclusion, while none of the patients had positive peritoneal cytology with Papanicolaou's method, the FISH technique detected p53 deletion in 32.1% of the peritoneal washing fluids and 17.9% of the peritoneal drainage fluids. The FISH technique had higher sensitivity in detecting free cancer cells compared to the conventional cytologic examination. With the FISH technique, p53 deletion detected in the peritoneal washing fluid was not associated with the prognosis of the patients but p53 deletion detected in the peritoneal drainage fluid was associated with positive radial resection margin more frequently and early peritoneal metastasis. Detecting p53 deletion with the FISH technique is an effective method to identify microscopic residual disease of resectable pancreatic cancer after curative intended resection. More aggressive systemic chemotherapy should be performed for patients with p53 deletion detected in peritoneal drainage fluid.





 XML Download
XML Download