

 ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Carcinoid tumors are rare tumors that display neuroendocrine properties. About 90% of carcinoid tumors arise in the gastrointestinal tract (GIT) [1]. Carcinoid tumor is the most frequent primary malignant tumor of the small intestine beyond the ligament of Treitz and most frequently arises in the terminal ileum [2,3]. Secondary mesenteric involvement of small bowel carcinoid tumors is common, reported as occurring in 40% to 80% of cases [3,4]. However, primary mesenteric carcinoid tumors are very rare and most solid tumors arising in the mesentery are usually metastatic tumors [1,2]. Distant metastasis rates from carcinoid tumors increases up to 80% to 90% when the size of the tumor is larger than 2 cm [3-5]. We present a very rare case of a primary mesenteric carcinoid tumor with 8.2 × 7.3 cm sized that demonstrated a benign character.
CASE REPORT
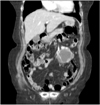
A 73-year-old woman presented with a palpable abdominal mass which had been increased in size for 1 year. She denied any other gastrointestinal or systematic symptoms. Physical examination revealed an 8 cm sized round and movable mass without tenderness in the periumbilical area. Computed tomography (CT) scan demonstrated an 8.2 × 7.3 cm sized well-defined mass with complex density located in the mesentery or adjacent proximal jejunum (Fig. 1).
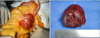
At laparotomy, a well-encapsulated mass was found to be arising from the small bowel mesentery near the ligament of Treitz (Fig. 2). We carefully dissected and removed the mass without injury to adjacent organs. There were no abnormal findings in the other organs including the small bowel and colon.
Histological examination showed tumor cells composed of homogenous small cells arranged in a trabecular pattern with the nucleus showing a round to oval shape, indistinct nucleoli, and coarsely granular chromatin pattern. There was no mitosis (Fig. 3A, B). Immunohistochemistry showed the tumor to be positive for multiple neuroendocrine markers including synaptophysin (Fig. 4A), CD56 (Fig. 4B), cytokeratin (Fig. 4C). Histopathologic examination confirmed the mass as a carcinoid tumor with a benign nature. At 11 months of follow-up, the patient was asymptomatic and recurrence free. This study had been approved by the Institutional Review Board of St. Vincent's Hospital, The Catholic University of Korea (VC12ZISE0142).
DISCUSSION
Carcinoid tumor is a rare, slow-growing, neuroendocrine tumor with about 90% of the lesions arising in the GIT [5]. GIT carcinoid tumors are classified by the embryologic origin as foregut, midgut and hindgut. 46% to 64% of GIT carcinoid tumors arise in the midgut and most midgut carcinoid tumors originate in the terminal ileum [3].
However, primary carcinoid tumors of the mesentery are very rare [2]. And carcinoid tumors arising in the mesentery are usually metastatic. Midgut carcinoid tumors commonly spread to the mesentery, reported as occurring in 40% to 80% of cases in various series [2].
On CT scan, mesenteric carcinoid tumors exhibit varying degrees of fibrosis, calcification, focal or diffuse neurovascular bundle invasion by the tumor or both mechanisms [2].
Surgical excision is a mainstay of treatment for carcionid tumor. Larger tumors are usually associated with locally advanced or distant metastasis [3]. Also, approximately half of midgut carcinoid patients present with liver metastasis [2]. Generally, for tumors smaller than 2 cm without lymph node involvement, local segmental resection is adequate [3,4]. And tumors larger than 2 cm with regional mesentery metastasis and lymph node involvement, wide excision of the bowel and mesentery with lymph node dissection is needed because tumors larger than 2 cm are associated with 80% to 90% incidence of metastasis [3-5]. Also, surgical debulking of local or distant metastatic carcinoid tumors is recommended, both for relief of symptoms and prolonged survival, despite randomized evaluation not being done [3-5].
Microscopically, typical carcinoid tumors have one of five growth patterns: insular, trabecular, glandular, undifferentiated, or mixed [3]. Most midgut carcinoids show a mixed insular and glandular growth pattern [4].
In this case, the tumor originated from the mesentery near the ligament of Treitz and well encapsulated, free from the small intestine (Fig. 2). At the time of surgery, the entire small bowel was meticulously inspected and no evidence of tumor mass or enlarged lymph node was found. In addition, there was no evidence of tumor anywhere else in the abdomen including the liver, ovary and other solid organs. So, it may be a primary mesenteric carcinoid tumor or metastasis from an occult primary site. Carcinoid tumors often have advanced malignant potential depending on location, size, nature. But this case shows a rare large primary mesenteric carcinoid tumor with characteristics of uncommon position and benign nature.


 XML Download
XML Download