

 ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Low anterior resection is the operation of choice for low rectal cancer, the formation of a straight anastomosis or colopouch anal anastomosis with total mesorectal excision is regarded the procedure of choice for such lesions [1,2]. However, the major complication of mesorectal excision is a significant anastomotic leak rate [3,4]. Anastomotic leak is a recognized complication of anterior resection with published rates varying from 2.8 to 25% [5,6].
A defunctioning stoma is recommended after low anterior resection for rectal cancer to decrease clinical anastomotic leak rate and reoperation rate [7]. Covering stomas are routinely closed at 8 to 12 weeks after the initial surgery. Before stoma closure, the distal anastomosis is routinely evaluated to rule out anastomotic leak or fistula formation by physical examination, proctoscopy, and radiographically by contrast enema. Previous studies have shown that contrast enema examinations are useful for detecting many of these complications before takedown of the diverting ileostomy. However, it is unclear whether this should be performed selectively or routinely.
The use of barium enema to confirm the anastomotic integrity prior to ileostomy closure is still controversial. The purpose of the study was to determine the utility of routine contrast enema prior to ileostomy closure and its impact on patient management in patients with a low pelvic anastomosis.
METHODS
One hundred forty-five patients had a temporary loop ileostomy constructed to protect a low colorectal or coloanal anastomosis following low anterior resection for rectal cancer between 2005 and 2010 from a single institution. All patients were evaluated by physical examination, proctoscopy, and barium enema prior to ileostomy closure. Patient demographics, radiographic imaging, and clinical course were reviewed and analyzed. Routine postoperative follow-up was a clinic visit 4 to 6 weeks after surgery at which time patients underwent clinical evaluation including a digital rectal examination and proctoscopy by two colorectal surgeons. Patients were then seen again approximately 3 months postoperatively at which time they were again evaluated by digital rectal examination and proctoscopy. After this clinic visit, each patient underwent radiographic evaluation of the distal anastomosis by contrast enema. If the anastomosis appeared intact and patent on examination, the patient was scheduled for ileostomy closure. The procedure was performed by a radiographer under fluoroscopic guidance. A 24-Fr Foley catheter was inserted via the patient's anus, and a sufficient amount of contrast was introduced slowly to distend and highlight the anastomosis and the proximal bowel. Postevacuation views were obtained for every patient. Contrast enema results were reviewed and compared with the information gained from patient symptoms and clinical examination.
Barium enema image before ileostomy closure was reviewed for radiographic signs of stricture or fistula at the ileoanal anastomosis.
The comparison was made to determine if routine contrast enema prior to stoma closure affected patient management.
RESULTS
One hundred thirty-eight patients underwent construction of a temporary defunctioning loop ileostomy to protect anastomosis. And 7 patients underwent construction of an ileostomy after anastomotic leak. One patients developed barium peritonitis due to iatrogenic bowel perforation during barium enema examination. Finally 144 patients were included in this study (Table 1). There were 83 men and 61 women with a mean age of 59.5 years (range, 28 to 87 years). Barium enema was performed and reviewed before the ileostomy closure. The median time from ileostomy creation to closure was 8 months.
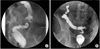
Five (3.5%) of the 144 patients were found to have clinically relevant strictures at the colorectal anastomosis on routine barium enema before ileostomy closure (Fig. 1A). The all strictures were resolved by digital rectal dilatation.
Of the 144 patients evaluated in this study, 1 patient (0.7%) showed anastomotic leak on their barium enema but he had no clinical signs or symptoms suggestive of clinical anastomotic failure (Fig. 1B). The patient was reversed without repeating the barium enema 1 month later and had an uneventful postoperative course.
Overall, 141 patients (97.9%) had an uncomplicated postoperative course. Postoperative complication occurred in 3 patients (2.1%). These patients are summarized in Table 2. One of them showed a stenosis on barium enema image and two had a normal finding.
DISCUSSION
The incidence of anastomotic leaks for colorectal anastomoses has been reported to range from approximately 3 to 12%. A loop ileostomy is constructed traditionally to reduce the septic consequences of anastomotic failure. A barium enema is done before ileostomy closure in order to evaluate the integrity of anastomosis and to confirm no evidence of any leak, stenosis or fistula. We analyzed the clinical usefulness of barium enema of the colorectal anastomosis prior to ileostomy closure.
In this study, it has been shown that the use of barium enema before ileostomy closure has no benefit in predicting postoperative colorectal anastomotic complications.
Only one (0.7%) of the 144 patients who had barium enema examination prior to ileostomy closure had a positive radiological finding of leak. This patient underwent ileostomy closure 1 month after examination because of nonspecific finding on pelvic computed tomography (CT) and had no problem in the colorectal anastomosis after operation. This rate was in accordance to other results in the literature. One study showed that the radiological leak rate was low where only 4 (5.9%) of the 69 patients had a positive radiological leak [8]. The other study showed no radiological leak on all patients who underwent anterior resection and defunctioning stoma formation [9].
Anastomotic stricture was the most common complication, especially in patients with cancer who had radiation therapy. In this study five patients showed stricture on radiologic imaging. Dolinsky et al. [10] suggested that the contrast enema is a more objective and reliable test for detecting strictures at the ileoanal anastomosis when a fixed threshold diameter is used. da Silva et al. [11] suggested that strictures may be reliably diagnosed by a simple digital rectal examination, and pouchogram does not contribute in diagnosing a clinically unsuspected stricture. In our cases, this problem could be detected clinically in the preoperative state as a result of routine pelvic examination, and managed nonoperatively by digital rectal dilatation. Therefore, it is not necessary to take a barium enema exam for finding out the anastomotic stricture after low anterior resection.
In our study, 3 patients developed colorectal anastomotic leak or abscess after operation. One of them showed a stenosis on barium enema image and two had a normal finding. The fact suggests that routine barium enema in the absence of a clinical suspicion of anastomotic failure would appear to be of little value. The patients were all male and presented with low or mid rectal cancer. The selective use of pouchogram at the time of suspicion for complications has been reported in two previous studies [12,13]. They showed pouchogram to be nonspecific and recommened CT scan to find a complication. In current study, it was difficult to predict who will develop postoperative anastomotic problem after ileostomy closure.
Furthermore, one patient had peritonitis due to perforation during barium enema examination. Barium peritonitis is reported to be related to a high morbidity and mortality [14], although currently mortality for adults seems to decrease mainly because of advances in medical care [15].
In case of an underlying septic lesion, excessive air insufflation during the procedure may aggravate the infection leading to haematogenous infection.
In this study, seven patients underwent ileostomy after anastomotic leak. These patients didn't show abnormal finding on preoperative barium enema and also didn't develop postoperative complication. This fact is contradictory to the previous study suggesting that preoperative barium enema should be considered in patients with an ileostomy constructed after anastomotic leakage [16].
In conclusion, routine contrast enema evaluation of low pelvic anastomoses before loop ileostomy closure did not provide any additional information for postoperative complication. And wheather an ileostomy is constructed during the first operation or after anastomotic leak was not related to the postoperative anastomotic problem. More study is necessary to find out the risk factor for the postoperative anastomotic complication.


 XML Download
XML Download