

 ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Esophageal atresia is one of the most significant congenital diseases in pediatric surgery, requiring prompt surgical treatment for optimal outcome in that its outcomes are mainly dependent on the surgery. Since the first successful repair in 1941 [1], treatments for esophageal atresia have gradually evolved due to not only better preoperative and postoperative neonatal intensive care but also the application of meticulous and precise surgical techniques [2]. Recently, the mortality rate associated with esophageal atresia was reported to be less than 10%, and high-risk neonates now have a better prognosis [3].
However, esophageal atresia is still a difficult disease for the pediatric surgeon who may not have sufficient experience. Postoperative complications such as anastomotic leakage and stricture are common, and occasionally, recurrence of tracheoesophageal fistula (TEF) occurs. Additionally, gastroesophageal reflux (GER) and esophageal dysmotility are often observed during long-term follow-up. These issues are currently under investigation [3].
In this study, we reviewed our experience regarding the treatment of esophageal atresia with or without TEF. As one of the large studies of esophageal atresia in Korea, our results may well contribute to improvements in treatment outcomes for esophageal atresia.
METHODS
We performed a retrospective review of the clinical data of patients who were treated for esophageal atresia at Severance Children's Hospital from January 1995 to December 2010. Cases prior to 1995 could not be included because of the incompleteness of the data. Overall, 107 patients were treated during the study period. Among them, 29 patients were excluded from the study because they did not undergo primary surgery at Severance Children's Hospital; instead, they were transferred from other hospitals after complication from the primary surgery. We also excluded six patients from the study because four patients were discharged against medical advice before surgery and two, who had severe multiple congenital anomalies, died immediately after birth.
We analyzed the data of 72 patients. The following data were collected: patient demographics including combined anomalies and types of esophageal atresia, diagnostic tools, methods of surgical procedures, and treatment outcomes.
Statistical analyses were performed using IBM SPSS ver. 18.0 (IBM Co., Armonk, NY, USA). Two-sample t-tests and chi-square tests were used to analyze the data, with P-values less than 0.05 considered significant.
RESULTS
Demographics
Patient characteristics are shown in Table 1. Fifty patients (69.4%) had combined anomalies, and VACTERL association with two or more anomalies was identified in 14 patients (19.4%). Among the combined anomalies, cardiac anomalies were most common (43 patients, 59.7%), and 12 patients (16.7%) had major cardiac anomalies that required surgery.
The most common gross type of esophageal atresia was C (59 patients, 81.9%), followed by types A (11 patients, 15.3%) and E (H-type, 2 patients, 2.8%). The other types were not found in our data.
Diagnosis
All patients with types A and C esophageal atresia were diagnosed by the identification of a coiled gavage tube by chest radiography. Two cases of H-type TEF were diagnosed by contrast esophagography. In 17 cases (23.6%), chest computed tomography (CT) was performed to evaluate the anatomy of the TEF and to measure the distance between the proximal and distal esophagus.
Surgical management
The surgical methods are summarized in Table 2. Most patients with type C esophageal atresia underwent repair by primary surgery (mean age, 3.9 ± 2.2 days), but seven underwent staged operations due to severe combined anomalies (4 patients) and long-gap atresia (3 patients). One of four patients with severe combined anomalies did not undergo definite surgery after gastrostomy because the parents declined further treatment early in the study. Three of four patients with severe combined anomalies were performed only gastrostomy in the first operation. Three patients with long-gap atresia underwent fistula ligation, gastrostomy, and cervical esophagostomy in the first operation.
All patients with type A esophageal atresia underwent staged operations, which included esophago-esophagostomy after elongation of the proximal and distal esophagus by several bouginations, adopted by the authors in 2004 [4].
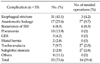
Postoperative complications
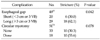
In 53 patients (73.6%), postoperative complications developed (Table 3). The most common complication was esophageal strictures that were mostly treated by esophageal balloon dilatation or bougination. However, in three cases, segmental resection of esophageal stricture and end-to-end anastomosis were performed. We were able to obtain data on the esophageal gap (distance between the proximal and distal esophageal end) in 49 patients and on circular myotomy in 51 patients (Table 4). Postoperative esophageal strictures developed more often in the long-gap than in short-gap atresia (P = 0.042). However, circular myotomy was not significantly associated with esophageal stricture (P = 0.078).
Anastomotic leakage was the second most common complication in our study. Only one case of anastomotic leakage required surgery, as the other cases were resolved by conservative management. However, among these cases, six patients (8.3%) were found to have delayed TEF recurrence. The mean date of TEF recurrence was 6.7 months (range, 0.6 to 23 months) after primary operations. One case of H-type esophageal atresia and two cases of long-gap type C atresia were included. All underwent another surgery.
Mortality
Overall, the mortality rate was 15.3% (11 patients). Eight patients died due to surgery-related complications, and two patients died after cardiac surgery. One patient with Down's syndrome died due to an unknown cause 1 year after surgery. The reasons for death due to surgery-related complications were leakage or recurrent TEF-induced respiratory failure (4 patients), postoperative sepsis with acute renal failure (3 patients), and hypoxic brain damage due to tracheomalacia (1 patient). If we include two patients who died immediately after birth, the mortality rate would increase to 17.6 % (13/74).
When comparing the mortality rate with the birth weight, the mortality rate of patients weighing less than 2.5 kg (34.6%, 9/26) was significantly higher than the rate of patients weighing at least 2.5 kg (4.3%, 2/46, P = 0.001).
Comparison of postoperative outcomes
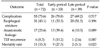
We grouped the patients into the early study period (from 1995 to 2003) and the late study period (from 2004 to 2010) based on an evenly balanced number of patients and the study duration.
In comparing the late period with the early period, patients in the late period had significantly lower rates of anastomotic leakage (P = 0.009) and mortality (P = 0.023) than those in the early period. However, the total complication rate, including esophageal stricture and recurrence of TEF was not significantly different between the two periods (Table 5).
DISCUSSION
Esophageal atresia is a complex congenital anomaly with a complicated prognosis. Although survival of patients with esophageal atresia has markedly improved due to advances in surgical techniques and neonatal intensive care, complications often occur, and morbidities after treatment are still regarded as an important issue [5,6].
The reasons for the high morbidity associated with esophageal atresia are well known [2,5,7,8]. Associated anomalies, low birth weight or prematurity, and likelihood of pneumonia are common findings with esophageal atresia and affect treatment outcome. In addition, variations in the type of atresia, anatomical differences, anastomotic tension induced by long-gap esophageal atresia, and lack of surgical experience are also considered as potential risk factors [6,7,9]. In this study, our results have shown that some of these factors are correlated with the postoperative prognosis. The incidence of complications is so high that 73.6% of patients have at least one complication. Postoperative esophageal strictures, which are the most common complication, were significantly correlated with the length of esophageal gap. Associated congenital anomalies are also common findings of esophageal atresia. Among them, major congenital heart disease, which is regarded as a prognostic factor, was one of the causes of death in this study.
Birth weight, another prognostic factor, is a valid factor in this study as well. Using the Waterston classification, a birth weight of 2.5 kg was used as one of the criteria to divide the patients into three groups [10]. Our data showed that patients weighing less than 2.5 kg at birth had a significantly higher mortality rate compared with patients weighing at least 2.5 kg at birth. Although these data were not analyzed by a multivariate analysis, they suggest that low birth weight is associated with poor prognosis, such as high incidence of associated anomalies, poor general physical status, and difficulty during the surgical procedure. However, these results are based on the data from the early period of the study. In the late period, we had only two cases of mortality with birth weights of 1.04 kg and 2.57 kg. Consequently, survival of patients in the late study period was not statistically associated with birth weight.
When we analyzed the data in early and late periods, significant improvements were found in the survival of patients in the late study period. Previous studies also showed that survival of esophageal atresia has gradually improved over past decades. Spitz et al. [11] emphasized that early diagnosis with improvements in neonatal intensive care and a number of surgical advances contribute to reductions in mortality; they revised the criteria for risk classification to be more tolerant of high-risk patients previously assigned using the Waterston classification. In addition, Poenaru et al. [12] proposed a new classification, the Montreal classification, which depends on the use of a ventilator and major combined anomalies. These new classifications attempted to define new risk factors and their association with the improved outcome. Although the timing of the early and late periods in this study is later than either the Spitz or the Montreal classification schemes, our results are supportive of improvements in outcome.
One interesting result of our study was the incidence of gross type A esophageal atresia. Usually, the incidence of type A atresia is less than 10%, but our data showed a relatively high incidence of type A (15.3%) [3,5,13]. Therefore, we used various surgical methods such as esophago-cologastrostomy (ECG), transhiatal gastric pull-up (THGP), and transthoracic esophago-esophagostomy after elongation (TEEE). Whether the esophagus should be preserved or replaced using either the stomach or colon, are still controversial [3,4,14,15]. Our outcomes after the different surgical methods were not analyzed statistically because of the few cases performed using each type of surgery. However, two of the three patients who received ECG died due to postoperative complications. The patients who received the other staged operations, THGP and TEEE, are still alive. Therefore, we suggest that staged operation using TEEE or THGP is better than ECG as a treatment for long-gap esophageal atresia, including type A. However, further research regarding the best choice of surgical method for either long-gap or type A esophageal atresia should be undertaken.
The other noticeable finding of this study is the use of chest CT for preoperative diagnosis. Traditionally, a diagnosis of esophageal atresia is not difficult. Simple insertion of a nasogastric tube and its coiling in the proximal esophageal pouch is a sufficient diagnostic method. However, recent studies report that a chest CT image with three-dimensional (3D) reconstruction provides preoperative information about the anatomy around the esophageal atresia, even the esophageal gap length. Therefore, CT imaging can help to determine the optimal surgical method [16-18]. We used a chest CT for the same reasons in 17 cases (23.6%). Our results could not confirm the effectiveness of the 3D reconstructed image in terms of the anatomy around the esophageal atresia and the esophageal gap. However, because the number of our CT performances was small, further research regarding the more established applications of chest CT imaging is needed.
In Korea, clinical studies of esophageal atresia are not common: only five reports with a large patient population were previously published [19-23]. When we analyzed those studies, our results were comparable regarding the high incidence of combined anomalies and the complication rates; however, one intriguing result was the incidence of GER (Table 6).
GER is a significant complication of the treatment of esophageal atresia: Seo et al. [20] reported the incidence of GER as 39.0%, and Kim et al. [21] reported it as 19.2%. According to the literature, GER occurs in approximately 40% of cases of esophageal atresia with approximately one-half requiring surgery [3,24,25]. In our study, GER developed in 4.2% of patients, and all were treated by conservative management. We could not exclude, however, underestimation of the incidence of GER because of the limitations of a retrospective study and an insufficient follow-up period.
In summary, our data suggest that the survival of patients with esophageal atresia has improved over the years and the rate of anastomotic leakage was significantly reduced. However, overall morbidities related surgical treatment of esophageal atresia still exists with high incidence. Further studies to reduce the surgical complications should be required.



 XML Download
XML Download