

 ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Familial adenomatous polyposis (FAP) is an inherited disease characterized by multiple adenomatous polyps in the colon and rectum. Multiple polyps are presented at a young age, and without treatment, they inevitably progress to colorectal cancer by the fourth decade [1]. Therefore, patients are usually treated by prophylactic total proctocolectomy in their teens or early twenties [2]. However, young patients who undergo an operation for FAP are socially active and cosmetically conscious. Therefore, the less invasive approach would be a favorable choice for FAP patients.
Total proctocolectomy with ileal pouch-anal anastomosis (TPC/IPAA) is the standard surgical procedure for the treatment of FAP. This procedure by open approach has been favored for its low morbidity, positive functional outcomes, and good quality of life [3,4]. Since the laparoscopic approach has been performed for various colorectal diseases, they have been applied in the treatment of FAP as well. However, early reports for laparoscopic TPC/IPAA failed to demonstrate significant benefits over the conventional open approach, because of its long operative time, high open conversion rates, and perioperative complications [5-7]. However, laparoscopic TPC/IPAA has been progressively developed and recent reports have demonstrated that laparoscopic TPC/IPAA is as technically feasible and safe as the open approach in selected patients [8-10].
Most FAP patients have benign polyps. However, it is practically impossible to perform histological examination on hundreds or thousands of polyps. Therefore, whether the polyps are benign or malignant, the surgeon should perform the operation according to oncological principles, such as regional lymphadenectomy and safe resection margin. A recent report found that the oncological safety of a laparoscopic operation in colorectal cancers was comparable to those of an open surgery [11]. However, there is doubt concerning the oncological safety of the laparoscopic approach for the treatment of FAP with coexisting malignancy.
In this study, we attempt to demonstrate the safety and feasibility of laparoscopic restorative total proctocolectomy by verifying its early postoperative and long-term outcomes. We also evaluated the long-term oncological outcomes in patients with FAP and coexisting malignancy.
METHODS
From August 1999 to September 2010, the prospectively collected records of patients who underwent TPC/IPAA or total colectomy/ileorectal anastomosis (TC/IRA) for FAP at Kyungpook National University were reviewed. All procedures were performed in a laparoscopic-assisted or hand-assisted laparoscopic surgery (HALS) manner. Colonoscopic examinations were performed in all patients, and biopsy results were consistent with adenomatous polyposis. If patients were diagnosed with adenocarcinoma with multiple adenomatous polyposes, they were staged using the clinical tumor-node-metastasis classification by computed tomography (CT), magnetic resonance imaging, or positron emission tomography-CT, if needed.
Surgical technique
All procedures were performed by a single surgeon (GSC). The patient was placed in a modified lithotomy, the Trendelenburg position, and right side down. One 12-mm infraumbilical port for the camera and four 5-mm trocars in each quadrant of the abdomen were introduced. First, the surgeon was positioned on the right side of the patients. High ligation of the inferior mesenteric vessels and full mobilization of the left colon were performed. The rectum was mobilized to dissect through an avascular plane with nerve-preserving technique as far distally as 1 to 2 cm above the dentate line, and the rectum was transected. The splenic flexure was fully mobilized while sparing the spleen. The surgeon continued the mobilization of the transverse colon to the right side, and ligated the middle colic vessels if possible. Second, the patient was placed left side down. The surgeon moved to the left side of the patient and dissected the colon from the ileocecal area to the hepatic flexure for mobilization, and then continued to meet the dissection point, which was mobilized at the left side. The right colic vessels were ligated, as well as the middle colic vessels, if not already ligated. The ileocolic vessels, however, were preserved to secure ileal pouch blood flow, except for the cases where a large polyp was situated at the right colon or was suspicious of a cancer. In initial cases, a 6 to 8 cm hand-port was placed in the Pfannenstiel incision above the symphysis pubis to mobilize the colonic flexures on both sides. The Lap-Disc (Ethicon Endo-Surgery Inc., Cincinnati, OH, USA) was covered to protect the wound.
After full mobilization of the colon and rectum, total colon was extracted through the Pfannenstiel incision or the right lower quadrant transverse incision as a protective ileostomy. Then, an approximately 15 cm length J-pouch of the ileum was made by linear staplers. For the ileal pouch to reach the anus without tension, the length of the ileal mesentery was extended by modifying the ileal vessels. IPAA was made according to the hand-sewn technique using 3-0 vicryl after rectal mucosectomy or the stapling technique using a circular stapler. If necessary, a diverting ileostomy was made.
In patients with synchronous liver metastasis, laparoscopic colorectal resection was performed first and then the liver was resected through the right subcostal incision using the open approach.
Postoperative follow-up
Patients were followed up annually. Clinical and endoscopic examinations were performed to evaluate the ileal pouch and anastomosis. Upper gastrointestinal examination was performed by endoscopy. Patients with FAP and coexisting malignancy received follow-up according to the cancer protocol. Patients classified as having stage II to IV cancer also received chemotherapy.
Statistical analysis
Data were analyzed using SPSS ver. 17.0 (SPSS Inc., Chicago, IL, USA). Fisher's exact test was used for comparing categorical variables. One-way analysis of variance with least significant difference was used to analyze the quantitative differences between three groups. Survival curves were generated using the Kaplan-Meier method and P < 0.05 was considered statistically significant.
RESULTS
Forty-three patients underwent laparoscopic operations for FAP during this period. Their median age was 33 years (range, 18 to 58 years). 27 (62.8%) had a family history of FAP; the remaining had no family history, but had over 100 adenomas, as determined by colonoscopic examination (Table 1).
Forty-one patients underwent TPC/IPAA. Of them, 33 patients underwent this operation by laparoscopic approach, and 8 patients by HALS. One patient, who was diagnosed by attenuated FAP with rectal sparing, underwent laparoscopic TC/IRA [12,13], and another 1 underwent laparoscopic TPC with end ileostomy due to extreme lower rectal cancer located at the dentate line, requiring abdominoperineal resection.
Intraoperative outcomes
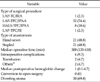
There were no conversions to open surgery. In 21 patients, the anastomoses were constructed using hand-sewn methods. All of them were made with diverting loop ileostomy, while 9 patients (20.9%) who had stapled anastomosis applied had diverting stoma (Table 2). The median operative time was 300 minutes (range, 135 to 610 minutes). The moving average learning curves for operative time are shown in Fig. 1. The learning curve decreased continuously with accumulation of experience, and reached a plateau after 22 cases. In this learning curve, 3 phases were classified by a turning point according to the operative approach or anastomotic methods. Comparisons of various parameters between the 3 phases are shown in Table 3. Phase 1 mainly consisted of the hand-assisted approach (including all 8 operations) and decreased on the operative times with repetition of the operation. Phase 2 consisted of a return to laparoscopic surgery; operative time seemed to increase initially, but decreased up to 22 cases, at which point it reached a plateau. With the introduction of a stapled anastomosis in our series and the increasing surgeon's experiences, the operative time stabilized in phase 3. Four intraoperative complications were observed; 2 cases of intraoperative bleeding that were resolved with blood transfusions, and 2 cases related to J-pouch formation.
Short-term complications within 30 days
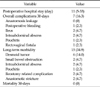
Seven patients (16.3%) experienced complications within 30 days (Table 4). One patient developed postoperative bleeding requiring reoperation, which was controlled by laparoscopic approach. Two patients experienced postoperative ileus, which was resolved after fasting and intravenous fluids. Two patients experienced intraabdominal abscess treated by percutaneous drainage. One patient developed pouchitis, which was treated by antibiotics. One patient developed a postoperative rectovaginal fistula, which required fistula repair by transanal approach.
Long-term complications
Two patients suffered from small bowel obstruction; 1 improved symptoms by conservative management and another required surgery. Two patients developed late intraabdominal abscesses due to blind-end J-pouch leakage treated by maintaining percutaneous drainage. The patient who developed pouchitis at 25 months postoperative was treated by conservative management. Two patients experienced anastomotic stenosis, which was resolved by anal dilatation. Two patients developed ileostomy reversal-related complication; postoperative anastomotic leakages. One patient was treated conservatively, while another had to have ileostomy reperformed (Table 4). During the follow-up period, 3 patients (7%) required reoperation for the aforementioned cause.
Six patients developed desmoid tumors; 5 in the mesentery, and 1 in the abdominal wall. One patient developed an intestinal obstruction by mesenteric desmoid tumors and was treated by surgical resection. No adenoma recurrences in pouch or anastomosis were found. All patients were subjected to upper gastrointestinal surveillance. 31 developed adenoma of the duodenum or ampulla, all of which were treated by endoscopic polypectomy.
Oncological outcomes of FAP patients with adenocarcinoma
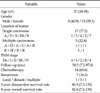
Twenty-two patients were diagnosed with colorectal malignancies (Table 5). The median age was 37 years (range, 24 to 58 years). Seventeen patients developed a single carcinoma and the remaining 5 developed multiple carcinomas. Four patients were Tis, but the remaining 18 developed carcinomas that were classified as greater than stage I. All patients with stage IV developed hepatic metastasis and underwent simultaneous hepatic resection with curative intent after laparoscopic colonic resection. The regional lymph nodes were harvested in abundance, and the upper and lower resection margin was also acquired in all cases. The median follow-up was 58.5 months (range, 7.2 to 97.8 months). Fourteen patients received chemotherapy. Seven patients developed recurrence; 5 had distant metastasis, 1 multiple metastases, and 1 local recurrence in the pelvic cavity. These 7 patients were treated with surgery, chemotherapy, or chemoradiotherapy (Table 6). Overall disease-free survival was 40.4 months (range, 7.2 to 135.5 months) and overall survival was 60.6 months (range, 7.2 to 135.5 months). Three patients died from pulmonary and hepatic metastasis.
DISCUSSION
This present study demonstrated that laparoscopic restorative total proctocolectomy for the treatment of FAP is safe and feasible, with acceptable early postoperative and long-term complications. In addition, this laparoscopic approach for treating FAP with coexisting malignancy gains oncological safety by optimal histopathological results and lower local recurrence rates.
Most FAP patients are young, and thus, socially active and cosmetically conscious. Despite these patient characteristics, TPC/IPAA consists of an extremely wide range of operation procedures, and very large incisional wounds, which not only cause damage to the body image, but also require a long time for recovery. From this perspective, a less invasive laparoscopic surgery would be a favorable alternative treatment for FAP patients. However, laparoscopic TPC/IPAA is a complicated and difficult procedure that combines all types of colonic operations. Furthermore, when colonic malignancy coexists, regional lymph node dissection and safe upper or lower resection margin must be secured for proper treatment. Therefore, greater experience and improved techniques are required for laparoscopic TPC/IPAA to be effective.
The early experience with laparoscopic TPC/IPAA did not show satisfactory results compared with open approach, owing to the longer surgical times, higher conversion rates, and increased complication rates [5,6]. Most of all, the biggest problem with the laparoscopic approach was excessive extension of time taken for operation. This is caused by the proportionality between time and area of operation because of the relative inexperience of the surgeon in laparoscopic operations. However, as observed in the learning curves that appear after the introduction of new operational procedures, the operative times showed a decreasing trend upon repetition of operations, which stabilized after 22 cases in the present study (Fig. 1). These results might be related to improved laparoscopic technique and accumulation of surgical experience [14]. In addition, after the plateau in the learning curve (22 cases), the operative time, which was 238 minutes (range, 135 to 385 minutes), was also comparable to the open approach for FAP in previous reports [8,15]. In addition, hospital stays and postoperative morbidity showed a decreasing trend after the surgeons gained sufficient experience in phase 3 (Table 4). Similar to our experiences, more recent studies for FAP have shown several advantages of the laparoscopic approach based on more experienced laparoscopic surgeons [16,17].
On a technical viewpoint, one of the difficulties is the isolation of the transverse colon from colonic flexures on both sides and dissection of the middle colic vessels. To overcome this, we created a Pfannenstiel incision of about 6 to 8 cm in the initial 8 cases. Operative time using HALS was shortened compared to earlier laparoscopic surgery; but in the later cases, we returned to normal laparoscopic operations after the expansion of laparoscopic surgery to treat all the colorectal diseases, including rectal cancer, using the experiences of over 250 cases of laparoscopic colorectal resection [14]. This was because HALS is associated with the possibility of an unnecessarily narrow operational view, and the possibility to dilute several advantages of the laparoscopic surgery because of excessive handling of the colon. Advanced laparoscopic instruments that enable easier hemostasis and ablation, such as ultrasonic dissector, also had a role in returning to laparoscopic surgery. However, if the surgeon is inexperienced in laparoscopic operations, HALS in some difficult parts of the operation may be useful. In the early period of the present study, operative time using HALS decreased sharply compared to the earlier laparoscopic surgeries (Fig. 1, from case 4 to case 11). In phase 1, the postoperative morbidity and hospital stays were rather shorter than those in phase 2, which occurred during the learning period although the results of HALS were inferior to the laparoscopic surgery after overcoming the learning curve (22 cases). Another technical difficulty is related to the creation of the J-pouch. J-pouch should go down to the perineum without tension, and thus sometimes requires the design of the ileal vessel. In the present study, to achieve sufficient mesenteric circulation, we created the J-pouch after first preserving the ileocolic vessel, unless there was the presence of a large polyp or suspicion of a cancer in the right colon [18,19]. Although 2 cases had the complication of vascular mobilization during J-pouch creation, we achieved adequate length of the J-pouch that could go down to the perineum without tension. We deemed this to be one reason why we did not experience anastomotic leakage through all cases.
IPAA can be performed by hand or an auto-suture stapler. The development of stapling techniques has greatly accelerated the speed of restorative proctocolectomy without detriment to the quality of continence [20,21]. The greatest impact of stapling instruments is in facilitating a safe IPAA such that a defunctioning ileostomy is not necessarily mandatory. However, in cases of coexisting rectal carcinoma or low rectal polyps, mucosectomy and sutured IPAA would still be the preferred procedure [22]. In present study, we preferred hand-sewn anastomosis with protective ileostomy in the early cases, because routine mucosectomy was executed to exclude any possibility of the development of rectal polyps. However, stapling was possible almost until the dentate line without functional impairment, and many reports have demonstrated that no recurrence occurs in the staple line or remaining rectal mucosa after stapling anastomosis [23]. Based on these results, in the later cases (Table 4, in phase 3), stapling anastomosis was preferred, except in cases requiring rectal mucosectomy. This change reduced the operative time by approximately 180 minutes (hand-sewn vs. stapled, 414 minutes vs. 230 minutes; data not shown), with a substantially lower creation rate of diverting stoma (hand-sewn vs. stapled, 100% vs. 33%). Long-term safety was also achieved after the staple technique such that the anastomotic or pouch adenoma did not occur during follow-up periods.
In present case, 16.3% and 34.9% of patients experienced varying degrees of early and long-term complications respectively, with similar rates in previous reports [8,24,25]. Two patients suffered from postoperative ileus and 2 developed small bowel obstructions after 30 days, but only 1 of them required operative treatment. The onset of desmoid tumors are related to surgical trauma. Although we expected a reduction in the incidence of desmoid tumors owing to minimally invasive approach, 14% of patients in this study developed desmoid tumors, with a similar rate in previous reports [26,27]. One of these patients developed a symptomatic intestinal obstruction from a mesenteric desmoid tumor and underwent surgical resection. All patients with desmoid tumors were administered antiinflammatory agents, hormonal agents, or systemic chemotherapy; no mortality was seen during the follow-up period. Additionally, 72.1% of the patients developed adenomatous polyps of the duodenum or ampulla, diagnosed at the early stage by our annual endoscopic surveillance. All of them were treated by endoscopic polypectomy.
When FAP is not treated, it inevitably proceeds to colorectal cancer. Furthermore, even when there seems to be no colorectal cancer, it is practically impossible to perform histological examinations on hundreds or thousands of polyps. Therefore, it would be appropriate to perform preemptive operations while complying with oncologic principles, especially with larger polyps. In the present study, there were 5 cases where colorectal cancer was diagnosed after operation. Recent reports found that curability and safety of laparoscopic operations in colorectal cancers was comparable to that of open surgery [11]. However, only a few cases of laparoscopic operations have been reported in the treatment of FAP with coexisting malignancy [28]. In the present study, a relatively high number of patients were treated with coexisting malignancy on varying sites. Eighteen cases were classified as greater than stage I, and all 18 were successfully treated. In pathological results, the regional lymph nodes were harvested in abundance, and the upper and lower resection margin was also acquired in all cases. As a result, during the relatively long follow-up period, an acceptable recurrence rate was achieved through patients with advanced tumors developing recurrence. Only 1 patient who had double primary rectal cancer developed pelvic recurrence. The relatively high success rates resulted from the accumulation of laparoscopic techniques, like optimal harvesting of regional lymph nodes and total mesorectal excision. In other studies, however, some surgeons used auto-suture staplers for dissection of all vessels; these staplers are difficult for accurate and wide-ranging dissection of the regional lymph node. Such a procedure is very risky for patients in whom the malignancy was not discovered during preoperative colonoscopic evaluation, but was elucidated after operation. In the present study, cancer with distant hepatic metastasis was discovered in 4 patients, who were treated with a combined hepatectomy for curative intent. There were no specific severe complications observed. Although additional studies with greater sample size are required to examine the oncological stability of laparoscopic TPC/IPAA for the FAP patients with coexisting malignancy, our study demonstrated acceptable oncological outcomes for this approach.
This study included a relatively large number of patients with FAP, and a coexisting malignancy, which was treated with laparoscopic TPC/IPAA. Based on our results, laparoscopic TPC/IPAA is a technically feasible treatment for FAP patients. Operation time can also be reduced by accumulation of surgical experience as well as the development and use of advanced laparoscopic instruments. When maintaining the oncological principle, laparoscopic TPC/IPAA for FAP with coexisting malignancy is considered oncologically safe. Therefore, we believe that laparoscopic TPC/IPAA is an optimal method for FAP with or without coexisting malignancy, although a comparative study with more cases is necessary to obtain results that are more precise.




 XML Download
XML Download