

 ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Recently, the widespread use of endovascular procedures for the treatment of abdominal aortic aneurysm (AAA) or aortic occlusive disease (AOD) has increased the proportion of OAS requiring supra-renal aortic cross clamping (SRACC) [1-3]. For the majority of patients undergoing open aortic surgery (OAS), proximal aortic control can be achieved at the infra-renal aorta. When OAS is selected for patients with juxta-renal aortic occlusion (JRAO) or para-renal AAAs, SRACC is essential for proximal aortic control during surgery [4,5]. Postoperative renal or abdominal visceral complications are important considerations in patients who undergo SRACC [6].
The assumed pathogenesis of renal or visceral complications includes ischemia/reperfusion injury of the renal or splanchnic organs, atheroembolism from the aortic wall around the renal or splanchnic artery ostia during aortic clamping or declamping, and hypotension due to perioperative hemorrhage. During the last few decades, many authors have reported improved surgical results after SRACC using prophylactic measures to reduce renal or visceral ischemia, improved surgical techniques, and postoperative care [7-9]. The purpose of the present study was to report the frequency and clinical course of postoperative renal and abdominal visceral complications following OAS requiring SRACC, and we attempted to identify risk factors for postoperative renal insufficiency (PORI).
METHODS
We retrospectively reviewed a database of 473 patients who underwent OAS due to AAA or AOD between October 2003 and February 2012 at a single institute. For this study, we included 66 consecutive patients (14%) who had undergone OAS requiring SRACC. OAS was performed through either a transperitoneal (n = 61) or thoracoabdominal (n = 5) approach. In patients requiring supra-celiac aortic cross clamping (SCACC), left medial visceral rotation was performed to expose the upper abdominal aorta. Prior to aortic clamping, heparin, mannitol (12.5 g/L) and/or furosemide (20 mg) were routinely administered intravenously. In cases where a longer aortic clamping time was expected, such as with type IV thoracoabdominal aortic aneurysm (TAAA), we infused cold heparinized saline into the renal orifices to induce renal hypothermia.
The methods of aortic reconstruction included aortic interposition, or aorto-biliac or bifemoral reconstruction using a prosthetic graft (Hemashield; Maquet Cardiovascular, Wayne, NJ, USA or GORE-TEX, W. L. Gore & Associates, Inc., Flagstaff, AZ, USA). In the cases of an infected aneurysm, we used cryopreserved aortic allografts in two patients and polytetrafluorethylene (PTFE) grafts in the other patients. In cases of type IV TAAA or supra-renal AAA, we formed a proximal aortic anastomosis using the inclusion technique between the beveled prosthetic graft and the proximal aorta including the celiac axis, superior mesenteric artery and right renal artery, and then left renal artery revascularization was separately performed (Fig. 1).
To identify risk factors for the development of PORI (defined as serum creatinine [sCr] ≥1.5 mg/dL in association with sCr ≥150% of preoperative level), we analyzed demographics (age, gender), preexisting comorbidities, indications for aortic surgery (aneurysm vs. JRAO), and intraoperative variables (renal ischemic time [RIT], aortic clamping site, renal protective measure, and concomitant renal artery reconstruction). RIT was defined as the time interval from SRACC to both renal artery reperfusions. In patients who underwent SCACC, postoperative hepatic and pancreatic enzyme levels were investigated in addition to sCr level. According to the suggestions of Michalopoulos et al. [10], hepatic dysfunction was defined as clinical jaundice associated with the level of hepatic enzymes (aspartate aminotransferase [AST]/alanine aminotransferase [ALT]) elevated to more than twice the norm. Postoperative acute pancreatitis was defined as elevation of the level of serum pancreatic enzymes (lipase and amylase) to more than three times the norm and a positive abdominal computed tomography scan [11].
Continuous variables are presented as mean ± SD and categorical variables are presented as frequencies (%). Binary logistic regression models were used to identify risk factors for PORI. Differences were considered significant when the P-value was less than 0.05. Patient survival after surgery was calculated using Kaplan-Meier analysis.
RESULTS
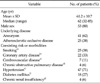
Among 473 OAS which performed during the study period, 66 patients (14 %; 53 males vs. 13 females; mean age, 61.2 ± 10.7 years; range, 32 to 85 years) required SRACC intraoperatively. The baseline demographics and coexisting risk and morbidities of the patients are summarized in Table 1.
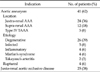
Four patients (7%) had preexisting chronic renal insufficiency (sCr ≥2.0 mg/dL), but no patients were on dialysis or had undergone kidney transplantation previously. Table 2 shows the surgical indications for aortic surgery requiring SRACC including 25 cases of JRAO and 41 aortic aneurysms (24 juxta-renal, 12 supra-renal and 5 type IV TAAA). Among the aortic aneurysms involving abdominal aorta, 15 (23%) were uncommon types of aneurysm which included 5 (8%) infected aneurysms, 4 (6%) inflammatory AAAs, 4 (6%) Marfan's syndrome and 2 (3%) Takayasu's arteritis. Four patients (9.8%) presented with a ruptured aortic aneurysm revealing normal blood
pressure (Table 2).
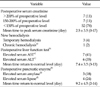
The sites of SRACC were the distal descending thoracic aorta in 2 patients (3%), supra-celiac in 15 patients (23%), supra-renal in 42 patients (64%) and inter-renal (aortic cross clamping between 2 renal arteries) in 7 patients (11%). Aortic reconstructions were performed using 12 patients (18%) prosthetic aortic tube grafts, 50 patients (76%) bifurcated grafts (48 prosthetic and 2 cryopreserved allografts), 2 aortic patch closures of the aneurysmal neck and 1 primary aortic aneurysmal neck closure. In a patient who had juxta-renal AAA with aortoduodenal fistula, aneurysm resection under the SRACC site was performed forming an aortic stump, followed by axillo-bifemoral bypass. With aortic reconstructions, 21 renal artery, 7 mesenteric and 1 hypogastric artery reconstructions were concomitantly performed. Details of the surgical procedures and adjunctive or concomitant procedures are summarized in Table 3.
The mean RIT was 30.1 ± 22.1 minutes (range, 3 to 120 minutes). Data for RIT were available in 61 patients (92%). The mean duration of RIT was 15.5 ± 1.4 minutes in JRAO, 35.1 ± 23.3 minutes in juxta-renal AAA (JRAA), 43.8 ± 21.6 minutes in supra-renal AAA (SRAA), and 51.3 ± 6.3 minutes in type IV TAAA. PORI developed in 14 of 66 patients (21%) (21% in JRAO, 21% in JRAA, 37% in SRAA and 21% in type IV TAAA). Four patients required HD, but chronic HD was required in one patient. The mean time to the postoperative peak level of sCr was 2.5 ± 3.5 days. Fig. 2 demonstrates scatter plots of postoperative sCr change according to the RIT. We found no correlations between postoperative sCr change and RIT (R2 = 0.166).
The elevation of hepatic or pancreatic enzymes was observed in 17 patients (26%) who underwent SCACC during the surgery. Though we have observed transient pancreatic (n = 7, 41%) and hepatic (n = 9, 53%) enzyme elevation after SCACC, there was no patients who shows diagnostic criteria of postoperative pancreatic or hepatic dysfunction suggested by Hashimoto and Walsh [11] and Michalopoulos et al. [10]. The serum pancreatic enzyme level returned to normal range within two weeks for all but one patient who exhibited prolonged elevation. Table 4 summarizes the postoperative blood test results for renal, hepatic and pancreatic enzymes. Fig. 3 shows the postoperative courses of serum AST, ALT, amylase and lipase levels.
On univariate analysis, SCACC (supra-celiac vs. infra-celiac aortic cross clamping, P = 0.035) and prolonged RIT (≥25 minutes vs. <25 minutes, P = 0.026) were predictors of developing PORI. However, they were not statistically significant for predicting PORI on multivariate analysis (Table 5).
There was one (1.5%) instance of operative mortality following aortic reconstruction in a patient with type IV TAAA infected with Listeria. Postoperative follow-up data was available in 82% of patients for a mean duration of 37.0 ± 31.9 months (range, 1 to 101 months). Patient survival at one, three, and five years after surgery was 90%, 79% and 79%, respectively (Fig. 4).
DISCUSSION
Endovascular aneurysm repair currently has a limited role for the treatment of aortic disease around the visceral-renal arteries. Therefore, OAS is still the gold standard treatment for patients with para-renal or para-visceral aortic disease. OAS is also challenging because it requires more extensive surgical exposure, has an increased risk of ischemic injury to renal and visceral organs or the spinal cord, and increased cardiac and pulmonary demands during SRACC. Therefore, OAS requiring SRACC carries a higher morbidity and mortality than infra-renal aortic surgery.
Greenberg et al. [12] recently reported excellent treatment results in patients with JRAA or TAAA using branched aortic stent grafts. However, the use of these devices is still not allowed in Korean or even in the United States, except in clinical trials. The results achieved by a few specialized centers cannot be generalized. As an alternative method to branched aortic stent grafting, aortic stent grafting with viscera and/or renal revascularization with a chimney technique can be used for the treatment of para-renal aortic aneurysms [13]. However, it remains to be determined whether the long-term results of the chimney procedure are equivalent to those of branched aortic stent grafting or OAS.
Since endovascular treatment for AAA and AOD are being more frequently performed, a greater proportion of OASs have become more complex [14]. Though the frequency of OAS requiring SRACC varies from center to center, it has a referral pattern to large centers. During the study period, 14% of patients undergoing OAS required SRACC in our hospital.
Some may argue against including type IV TAAA as an AAA. Though it is classified as a type of TAAA, it is apparent that type IV TAAA does not affect the thoracic aorta, but it does affect the abdominal aorta. Therefore, we included type IV TAAA as an AAA requiring SRACC.
Renal insufficiency is one of the most serious complications after SRACC. The reported incidence of PORI after OAS requiring SRACC ranges from 7.9 to 38%, which depends on the definition of PORI [15,16]. In this study, 21% (14/66) of patients developed PORI, which was defined as sCr elevated greater than 50% over the preoperative level. New HD was required in 4 (6%) of these patients; however most required temporary HD, while one patient (1.5%) who developed chronic renal failure required chronic HD. That patient presented with ruptured type IV TAAA and preexisting renal insufficiency. Numerous authors have reported that PORI develops more often in females, and patients with preoperative renal insufficiency, intraoperative hypotension, concomitant renal artery reconstruction and prolonged RIT [17-20]. In the present study, SCACC and RIT ≥25 minutes were identified as risk factors of PORI on univariate analysis.
The optimal site of aortic cross clamping is usually determined by the extension of the aortic lesion, associated arterial disease requiring concomitant repair, body habitus, etc. Green et al. [21] reported that SCACC carries a lower risk of PORI than aortic clamping just proximal to the renal arteries, which can prevent atheroembolism from the para-renal aortic lesion. Shortell et al. [17] also reported the merit of SCACC in patients with JRAA, including a reduced incidence of complications related to proximal aortic cuff disease. However, many previous authors have reported that SCACC is an independent predictor of PORI [20,22]. At our institution, we prefer aortic clamping at the inter-renal or supra-renal aorta to supra-celiac aorta, unless there is significant aortic calcification or mural thrombus around the renal artery orifices.
In addition to atheroembolism, acute tubular necrosis due to interruption of renal perfusion is a well-known pathogenesis of PORI. In an experimental rat model of renal ischemia, renal blood flow to the outer medullary area decreased dramatically during the first 30 minutes of renal ischemia and showed transient recovery to 50% of baseline blood flow for a three-hour period [23]. Prolonged RIT is a well-known independent risk factor for PORI. However, tolerable time duration to irreversible damage of the renal tissue was not well established after renal perfusion was stopped. Wahlberg et al. [18] reported the frequency of PORI according to the total RIT. According to them, PORI was very rare when the RIT was shorter than 25 minutes. The odds ratio increased to 2.2 (95% confidence interval [CI], 0.5 to 8.8) and 12 (95% CI, 1.0 to 141.3) when RIT lasted 26 to 50 minutes and >50 minutes, respectively. In the present study, RIT >25 minutes was a significant predictor of PORI on univariate analysis, but not on multivariate analysis.
Various protective measures and adjunctive surgical procedures are performed to reduce renal or visceral ischemic injury in patients with supra-renal or type IV TAAA. Though Cochrane Collaboration [24] recently reported that there is insufficient evidence to support the routine use of renal protective measures during aortic surgery, renal parenchymal cooling by the infusion of cold solution into the renal artery and prophylactic intravenous administration of mannitol and/or furosemide are frequently used to reduce renal ischemic injury. Our policy is to administer mannitol and furosemide intravenously before SRACC, and to infuse cold heparinized solution into the renal artery when prolonged RIT is anticipated. A typical example is cooling of the left kidney when a separate left renal artery reconstruction is planned after the completion of proximal aortic anastomosis. According to Knott et al. [19], 12% of juxta-renal AAA patients required renal artery revascularization during OAS. In the present series, renal artery revascularization was performed in 29% of patients who required suprarenal aortic clamping during OAS. These findings are similar to those of Chong et al. [7] who found the frequency of concomitant renal artery revascularization was 32% in patients who underwent OAS requiring SRACC.
SCACC is required in cases of type IV TAAA and some cases of suprarenal AAA. The amount of blood flow to the gastrointestinal tract, splanchnic organs and both kidneys is known to account for 55% of cardiac output [25]. Therefore, SCACC causes an increased cardiac afterload in addition to the renal, splanchnic and lower extremity ischemia. Major adverse effects can occur with SCACC, resulting in ischemia-reperfusion injury of the visceral organs. One of the most dreaded complications after prolonged SCACC is the development of intraoperative bleeding. Anagnostopoulos et al. [26] described the mechanisms underlying intraoperative bleeding tendency in an animal model that underwent SCACC for longer than 30 minutes. They explained that these mechanisms involved systemic intravascular thrombosis resulting in consumption coagulopathy and decreased fibrinolytic activity ("fibrinolytic shutdown") following ischemia-reperfusion of visceral organs. Hepatic hypoperfusion can cause decreased clearance of tissue plasminogen activator (t-PA) in the liver while increased t-PA production by the ischemic gut. Nypaver et al. [27] reported that postoperative complications related to organ ischemia developed in 14% of patients who underwent SCACC longer than 45 minutes during an elective OAS concomitant with renal or visceral artery revascularization.
Acute pancreatitis is a very rare complication after OAS [28]. The possible mechanisms of acute pancreatitis after SCACC include systemic or regional hypoperfusion of the pancreas, atheroembolism of the arteries supplying the pancreas, and mechanical injury to the pancreas. However, clinical features of postoperative pancreatitis can be obscured due to abdominal wound pain and gastrointestinal dysfunction in the immediate postoperative period. When we adopted the elevation of serum pancreatic enzymes by three times or more compared to the preoperative level as the definition of postoperative pancreatitis, the incidence was very rare after SCACC. Though SCACC can cause visceral organ ischemia, morbidity due to splanchnic organ hypoperfusion is often reported to be minimal [29,30]. Elevation of pancreatic and/or hepatic enzymes was observed after SCACC, but most returned to normal levels within two weeks.
To summarize our observations, OAS requiring SRACC or SCACC can result in renal or visceral complications. However, if the RIT is shorter than 25 minutes, SRACC is considered a safe procedure. Though we were unable to identify independent risk factors for PORI, we found that preexisting renal disease can progress to chronic renal failure after SRACC. We have encountered good short-term and long-term results after OAS with supra-renal or SCACC.






 XML Download
XML Download