

 ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Despite its decreasing global incidence over the past few decades, gastric carcinoma remains one of the most common malignancies in many East Asian countries [1]. In Korea, gastric carcinoma is the most prevalent malignant neoplasm and continues to affect over 2,500 patients per year [2]. However, with widespread implementation of screening programs, early gastric cancer accounts for nearly 50% of all gastric cancers, and 5-year survival has reached up to 63 to 73% after curative resection [3-5]. Given advances in the treatment techniques and the early diagnosis of gastric cancer, proper management of functional and nutritional impairments after gastric cancer surgery has also become a primary treatment concern in gastric cancer [6].
Postsurgical anemia is frequently encountered during the early postoperative period after gastrectomy and may impair physical performance and postoperative recovery. However, no standard care for postsurgical anemia, such as, concerning the use of iron or the best route for iron supplementation, has been established so far [7,8]. In the studies regarding orthopedic or cardiac surgery, oral or intravenous iron supplementation showed little efficacy for postsurgical anemia [9-12]. However, unlike patients undergoing orthopedic or cardiac surgery, patients with gastrectomy inevitably suffer from poor iron absorption from the gastrointestinal tract, and thus, this may adversely affect the physiologic recovery from postsurgical anemia [13]. Therefore, the use of iron supplementation for postsurgical anemia needs to be further evaluated in the subset of patients undergoing gastrectomy.
To facilitate proper management of postsurgical anemia, a comprehensive understanding about its clinical features is essential. Its prevalence, subsequent evolution, and the factors affecting the recovery should be taken into consideration when planning a treatment for postsurgical anemia. Therefore, we investigated clinical features of postsurgical anemia after gastrectomy, and sought to identify clinicopathological factors that affect its subsequent recovery.
METHODS
Patients
Between August 2008 and September 2009, 649 patients underwent curative surgery for gastric carcinoma at our institute. Of these patients, 198 patients that underwent preoperative or postoperative chemotherapy, 12 with combined resection of other organs, and 40 that experienced disease recurrence during the follow-up were excluded. Finally, 406 patients that received gastrectomy alone for the treatment of gastric carcinoma and followed for at least one year after surgery were enrolled in the present study. Patient data, such as, demographic characteristics, pathologic results, operative details, postoperative morbidity and mortality, and hospital courses were prospectively constructed using our electronic database recording system.
Postsurgical anemia was defined according to the World Health Organization definition based on hemoglobin (Hgb) value (Hgb < 13 g/dL for males and < 12 g/dL for females). The severity of anemia was also classified as mild (Hgb ≥ 10 g/dL), moderate (7 g/dL ≤ Hgb < 10 g/dL), or severe (Hgb < 7 g/dL) based on postoperative Hgb concentration [14].
During the follow-up, all patients were monitored until 12 months post-surgery, with regular blood test on 3, 6, and 12 months post-surgery. No specific treatment was given to patients with postsurgical anemia. Instead, additional laboratory test for iron deficiency, including serum iron and ferritin and total iron biding capacity, was carried out when patients showed microcytic or hypochromic anemia on regular blood test from postoperative 3 months, and oral iron supplementation was indicated only for postsurgical anemia with an evidence of iron deficiency. Consequently, 11 patients received oral iron supplementation during the follow-up.
Operative procedures and perioperative care
Distal or total gastrectomy with regional lymph node dissection was performed in all patients. D2 lymph node dissection, as outlined by the Japanese Gastric Cancer Association, was the standard procedure used for advanced gastric cancer, and D1 plus beta lymph node dissection the standard procedure for early gastric cancer [15]. Laparoscopic surgery was indicated for patients with a preoperative diagnosis of cT1-2N0 gastric cancer. Billroth I reconstruction was the primary procedure used after distal gastrectomy, and Billroth II or Roux-en Y gastrojejunostomy when gastroduodenostomy was not feasible because of concerns about anastomosis failure or the need for wide stomach resection. Roux-en Y esophagojejunostomy without a pouch, was performed routinely after total gastrectomy.
Patients were perioperatively managed using a standardized clinical pathway protocol. For example, no preoperative bowel preparation or nasogastric tube was used. Patients were administered an oral diet from postoperative day 1, and intravenous fluid was restricted to 20 to 25 mL/kg/day during the first three postoperative days. Prophylactic antibiotics were administered before skin incision and continued until 12 hours after surgery. Laboratory tests, such as, complete blood cell counts and blood chemistry, were regularly performed on postoperative days 1, 3, and 5. Transfusion was indicated for anemia with Hgb concentration of <6 g/dL or active postoperative bleeding [16]. Hospital discharge was targeted for postoperative day 8, and objective discharge criteria were used to make decisions, that is, no sign of postoperative complications, the ability to ambulate without assistance, tolerable pain on oral analgesia, able to consume more than 70 per cent of meals, and a willingness to go home.
Statistical analysis
Continuous data were converted into means (standard deviations [SDs]) and analyzed using the Student's t-test. The chi-square test was used to analyze categorical data. When analyzing risk factors, continuous data were dichotomized into categorical data, which enables the chi-square test and logistic regression analysis to be used for univariate and multivariate analysis, respectively. All statistical analyses were performed using SPSS ver. 12.0 (SPSS Inc., Chicago, IL, USA). P-values of < 0.05 were regarded statistically significant.
RESULTS
Patient characteristics
The demographic and treatment characteristics of the 406 patients are summarized in Table 1. The study subjects consisted of 265 males and 141 females of mean age (SD) 61.8 (11.2) years. One hundred and fifty five (38.2%) had underlying medical comorbidities at the time of operation. Distal gastrectomy was performed in 342 (84.2%), and total gastrectomy in 64 (15.8%) patients. Laparoscopic surgery was performed in 222 (54.75%) patients. Based on final pathologic examinations and the seventh edition of the Union for International Cancer Control tumor-node-metastasis classification, there were 326 stage IA and 80 stage IB patients.
Prevalence and severity of postsurgical anemia
Postoperatively, 318 (78.3%) patients presented with postsurgical anemia, and these included 30 (7.4%) patients with a postoperative bleeding complication. Mean estimated intraoperative blood loss (mL) was 175 ± 39, and mean change in Hgb concentration immediately after surgery was 2.3 ± 1.4 g/dL. Forty one (10.1%) patients received a blood transfusion postoperatively. Because we sought to monitor the postoperative recovery of serum Hgb level from the baseline level at the time of discharge, we decided to include the patients receiving perioperative blood transfusion based on their last blood test results. Finally, at the time of discharge from hospital (based on the last blood test before discharge), 271 (66.7%) patients had mild and 47 (11.6%) had moderate postsurgical anemia, but no patient had severe anemia.
Risk factors for developing postsurgical anemia
Of the 341 patients without preoperative anemia, 253 (74.2%) developed postsurgical anemia. Table 2 summarizes the risk factors of developing postsurgical anemia in patients without preoperative anemia. Univariate analysis showed that old age, female sex, lower body mass index (BMI), open surgery, D2 lymph node dissection, and total gastrectomy were significantly associated with the development of postsurgical anemia after gastrectomy. As for reconstruction types, Roux-en Y esophagojejunostomy was significantly related to the development of postsurgical anemia, but patients with distal gastrectomy showed no significant difference of postsurgical anemia according to the reconstruction techniques (P = 0.589, Fisher's exact test). Therefore, reconstruction type was excluded in the multivariate analysis. Multivariate analysis revealed that old age (≥60 years; odds ratio [OR], 1.87; 95% confidence interval [CI], 1.10 to 3.16), a female sex (OR, 1.89; 95% CI, 1.05 to 3.40), lower BMI (< 23; OR, 2.26; 95% CI, 1.21 to 4.24), and total gastrectomy (OR, 6.61; 95% CI, 1.95 to 22.41) were independent risk factors of developing postsurgical anemia after gastrectomy.
Evolution of postsurgical anemia during follow-up
Table 3 present postoperative courses of postsurgical anemia up to 12 months post-surgery. Of the 318 patients with postsurgical anemia, 173 (54.4%) achieved a spontaneous recovery at 3 months post-surgery without specific treatment. Patients with mild postsurgical anemia showed significantly better spontaneous recovery by 3 months post-surgery than those with moderate postsurgical anemia (59.4% vs. 25.5%; P < 0.001). However, no significant change in the recovery of postsurgical anemia was observed at 6 or 12 months postoperatively for both patient groups with mild and moderate postsurgical anemia. During the follow-up, only 11 (3.5%) of 318 patients with postsurgical anemia showed microcytic or hypochromic anemia with iron deficiency based on the blood test from the postoperative 3 months, and received oral iron supplementation.
Interestingly, of the 88 patients that did not develop postsurgical anemia after operation, only 9 (10.2%) newly developed anemia by postoperative 3 months, and 6 of them presented with anemia until 12 months post-surgery.
Factors affecting the recovery of postsurgical anemia
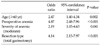
As we mentioned earlier, 11 postsurgical patients with iron deficiency received oral iron supplementation during the follow-up, and thus these patients were excluded from the analysis of factors affecting the recovery of postsurgical anemia to exclude the effects of iron treatment. Table 4 presents a summary of our analysis of predictors of persistent postsurgical anemia by 12 months postoperatively. According to univariate analysis, old age, the presence of preoperative anemia, severity of anemia (moderate), reconstruction type, and total gastrectomy were significantly associated with persistent postsurgical anemia by 12 months. In the subgroup analysis of patients with distal gastrectomy, there was no significant difference in the recovery of postsurgical anemia between different types of reconstruction procedure (P = 0.140, fisher's exact test). Finally, multivariate analysis revealed that old age (≥60 years; OR, 2.47; 95% CI, 1.40 to 4.34), preoperative anemia (OR, 4.87; 95% CI, 2.48 to 7.96), moderate postsurgical anemia (OR, 2.19; 95% CI, 1.03 to 4.63), and total gastrectomy (OR, 4.14; 95% CI, 2.15 to 7.97) were independent risk factors that adversely affect the spontaneous recovery of postsurgical anemia (Table 5).
DISCUSSION
Postsurgical anemia is common postoperative sequel during the early postoperative period after gastrectomy, and probably adversely affects physical performance and recovery. However, no clear consensus has been reached regarding the treatment of postsurgical anemia after gastrectomy, such as, whether to use iron or to determine the optimum route of iron supplementation [17]. The proper management of postsurgical anemia after gastrectomy may be best approached from a comprehensive understanding of its clinical features, but little is known about this condition. This study was performed as a pilot study for planning a treatment of postsurgical anemia after gastrectomy. In this study, we found that nearly 40% of patients with postsurgical anemia achieved a spontaneous recovery at 3 months post-surgery, but after then no significant recovery was observed until postoperative 12 months. This may suggest that spontaneous recovery of postsurgical anemia can be expected until 3 months post-surgery, but proper intervention may be required for postsurgical anemia persisting until 3 months postsurgery. However, no studies have evaluated proper treatment of postsurgical anemia, such as the efficacy of iron supplementation or the best route of iron supplementation, in patients undergoing gastrectomy. Therefore, proper management for postsurgical anemia needs to be further evaluated in further clinical trials.
In the present study, old age, preoperative anemia, severity of anemia (moderate anemia), and total gastrectomy were found to be independent factors adversely affecting the recovery of postsurgical anemia. This is probably because elderly patients or patients that undergo total gastrectomy are more likely to suffer from iron malabsorption due to poor oral intake and malnutrition [18,19]. Furthermore, patients with preoperative anemia possibly have underlying predisposition for the development of anemia. Therefore, our study suggests that the treatment of postsurgical anemia may require tailored approaches for these patients, such as an earlier active intervention or intravenous iron supplementation rather than oral supplementation. However, this also should be evaluated by clinical trials.
The treatment of postsurgical anemia, especially with respect to the efficacy of postoperative iron supplementation is an issue of long-standing debate [6,7]. Inflammatory response after surgery reduces serum iron and transferrin and increases serum ferritin, which is indicative of a state of functional iron deficiency [20,21], and these physiologic changes may negate the effects of iron supplementation during the postoperative period. In fact, several studies have failed to identify a benefit of iron supplementation for the treatment of anemia after non-abdominal surgeries [9-12]. However, unlike patients undergoing orthopedic or cardiac surgery, patients with gastrectomy inevitably suffer from poor iron absorption from the gastrointestinal tract, and thus, this may adversely affect the physiologic recovery from postsurgical anemia [22]. These arguments urge that the efficacy of iron supplementation during the treatment of postsurgical anemia and the optimal route of iron supplementation needs to be determined in patients undergoing gastrectomy.
It is well known that iron absorption is impaired in a multifactorial manner after gastrectomy, and reduced food intake, low gastric acidity, rapid gastric emptying, and bypass of the upper gastrointestinal tract have all been reported to contribute [22]. However, the extent and clinical consequences of iron malabsorption have not been fully investigated. In the present study, only six of 88 patients that did not develop postsurgical anemia developed anemia at 12 months postoperatively. This observation suggests that iron metabolism is relatively well conserved in normal patients despite gastrectomy. Turnberg [23], in a experimental study of iron absorption in patient with gastrectomy, found that iron absorption was greater in a gastrectomy group than in a non-anemic control volunteer group. Kimber et al. [24] also concluded that iron malabsorption does not necessarily follow gastrectomy. Based on these previous studies and our results, we consider that the extent of iron malabsorption after gastrectomy is less likely to result in impaired hematopoiesis in normal patients, but that it has a serious impact on the physiological compensation required for recovery from postsurgical anemia.
Old age, lower BMI, and total gastrectomy were independent risk factors of developing postsurgical anemia after gastrectomy. It may be due to the increased risk of intraoperative bleeding or increased vulnerability to hemodilution by perioperative intravenous fluid administration in the patients with these characteristics. The amount of intraoperative bleeding is undoubtedly the most important factor for developing postsurgical anemia. However, accurate measurement of the amount of intraoperative bleeding is seldom available in many clinical settings and sometimes even inconvincible. Therefore, we could not include the amount of intraoperative bleeding in our study, and thus independent risk factors, like old age, lower BMI, and total gastrectomy, are possibly related the intraoperative or postoperative bleeding rather than its independent correlation with the development of postsurgical anemia. However, under the clinical circumstances where accurate measurement of intraoperative or postoperative blood loss is not readily available, these factors can be used to predict the risk of developing the postsurgical anemia after gastrectomy.
In summary, based on our results, a spontaneous recovery of postsurgical anemia can be expected until 3 months post-surgery, but proper intervention may be required for postsurgical anemia persisting until postoperative 3 months. In addition, factors adversely affecting the recovery of postsurgical anemia should be taken into consideration in treatment planning for postsurgical anemia. Considering the differences in postoperative physiology of iron metabolism in patients undergoing gastrectomy, proper treatment of postsurgical anemia, such as the efficacy of the use of iron or the optimum route of iron supplementation, needs to be further evaluated in future clinical trials.




 XML Download
XML Download