

 ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The existence of sentinel lymph node (SLN) was demonstrated in penile cancer treatment by Cavanas from the study of lymphangiography and surgical experience [1]. On the basis of the SLN concept, SLN mapping and biopsy are now becoming standard procedures for early stage breast cancer and malignant melanoma [2-4]. The sentinel node concept also appears to be applicable to early gastric cancer, and SLN detection may contribute to minimally invasive surgery, selective lymphadenectomy, and accurate staging [5]. Therefore, SLN mapping and biopsy examination can reduce operative morbidity, mortality, and complication, now has become standard practice for early stage breast cancer and malignant melanoma [3,6,7].
The general method of SLN mapping is a radiocolloid scintigraphic method with intra-operative gamma probe counting [8]. However, that method cannot be used to predict the accurate anatomic location of primary SLNs preoperatively because the resulting images have limited spatial resolution, which means that the detailed anatomy of surrounding structures cannot be sufficiently visualized [5,9-11]. Detection of high-uptake lymph nodes adjacent to the injection sites is difficult owing to the shine through phenomenon [5,9].
The concept of computed tomography (CT) closely matches that of sentinel node mapping. Small-sized contrast media injected submucosally can reach lymphatic vessels owing to the increased permeability of the fenestrated endothelial lining of distal capillaries [12]. Similarly to radio-isotopes, such agents then follow the lymphatic flow and progressively converge towards afferent nodes. Wisner et al. [13] have assessed on CT imaging the behavior of locally administered iodinated contrast material whether injected in subcutaneous or within gastric mucosa.
CT lymphography is a safe technique with favorable results that allows sentinel node navigation for some malignancies [14,15]. This modality is also easy and inexpensive, requiring only a short time during routine CT to evaluate distant metastasis; thus, resulting in successful SLN navigation while saving time and cost. Iopamidol and lipiodol are possible agents to visualize the lymphatic pathway during CT lymphography, but injection of contrast media into organs or tissues can cause inflammation and a tissue reaction. Frozen sections during a gastrectomy are important for treating gastric cancer, because they reduce the risk of tumor recurrence. Thus, injection of contrast media can create confusion when examining frozen sections. These difficulties interpreting a frozen section are an obstacle when performing a gastrectomy.
The literature remains limited to direct visualization of sentinel node using contrast media in animal studies, and tissue reaction after injection of contrast media still have to be conducted to apply the CT lymphography on clinical practices.
METHODS
All procedures were performed under a protocol approved by the Guidelines for Animal Experimentation of Seoul National University Bundang Hospital.
Materials
Studies were conducted in adult (8-week-old, 18 to 20 g) female C57BL/6NCrj mice (Charles River Japan Inc., Yokohama, Japan). The mice were maintained in a light-and-temperature-controlled environment (14-h light, 10-h dark cycle, 22 to 25℃) and allowed a 2-week period of acclimation to the vivarium before any procedure was performed. Total ninety mice are used. The mice are divided into 3 groups. The animals fasted at least before and 12 hours after surgery. Two main groups of 30 mice received contrast agents. One group of 30 mice received isotonic saline. Two contrast agents and normal saline for negative controls were tested:
Methods
The mice are anesthetized with ketamine (60 mg/kg) and xylazine (8 mg/kg) by subcutaneous injection. The stomach is exposed by a 1 cm upper midline incision. A 30 gauge syringe is inserted into the submucosa, lesser curvature of antrum under microscopy. After injection of contrast agents or normal saline, upper midline wounds are closed by 4-0 prolene. Dissections are performed in 5 animals in each contrast media group postoperative day (POD) 1, 3, 7, 14, 28, 56 after injection. No antibiotics were administered during the study. Of each animal gastric specimen for histology were obtained.
Microscopic sections are taken from the harvested stomach. The sections are hematoxylin-eosin stained. Histologic reactions are evaluated according to type and severity of edematous or inflammatory reaction. Acute and chronic inflammatory reactions were graded (0 to 3) for leukocyte and lymphocyte infiltrations, respectively [16].
For grading of histologic reaction the system was used (Fig. 1):
Also, grading systems of fibrosis are categorized as following:
The presence or absence of fibrinoid necrosis, mesothelial hyperplasia, foreign body reaction to injection material, and uptake of contrast medium on high resolution X-ray examination using mammography were also evaluated to distinguish the difference between injection materials.
Statistical analysis
The SPSS ver. 11.0 (SPSS Inc., Chicago, IL, USA) was used for statistical analysis. Comparisons were made using the one-way analysis of variance (ANOVA) with Tukey post hoc analysis for multiple comparisons, independent t-test and chi-square test at each time point. Statistical significance was defined as P < 0.05.
RESULTS
There were 3 mortalities after operation. One mouse died of unknown cause after injection of normal saline at POD 54, and another 2 mice in iopamidol group were killed by cannibalism at POD 20 and 47, respectively.
Gross observations
Adhesions were either viscera-to-viscera, viscera-to-solid organ, or viscera-to-omentum. There was no gross evidence of peritonitis in any of the groups, although macroscopic abscess formation was seen in two rats, one with a lipiodol-injected and one control animal, at 1 week and 2 weeks, respectively.
Microscopic observations
Acute inflammatory reaction
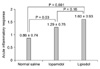
A comparison of mean grade of acute inflammatory reaction of harvested stomach after injection is provided in Fig. 2. No significant difference of mean grade was observed between iopamidol and lipiodol group. However, the mean grade after injection of lipiodol and iopamidol was significantly higher than control group (iopamidol vs. normal saline; 1.29 ± 0.76 vs. 0.86 ± 0.74, P = 0.03, lipiodol vs. normal saline; 1.60 ± 0.93 vs. 0.86 ± 0.74, P = 0.001).
Chronic inflammatory response
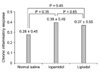
The mean grade of chronic inflammatory response caused by injection of normal saline, iopamidol, and lipiodol was the similar for all the time period (0.28 ± 0.45, 0.39 ± 0.49, 0.37 ± 0.55, P = 0.65) (Fig. 3). There were no significant difference between groups using independent t-test (normal saline vs. iopamidol, 0.28 ± 0.45 vs. 0.39 ± 0.49, P = 0.35; normal saline vs. lipiodol, 0.28 ± 0.45 vs. 0.37 ± 0.55, P = 0.49; iopamidol vs. lipiodol, 0.39 ± 0.49 vs. 0.37 ± 0.55, P = 0.85).
Fibrosis
There was no significant difference between groups in mean grade of fibrosis (0.97 ± 1.08, 1.04 ± 0.88, 1.10 ± 0.80, P = 0.85) (Fig. 4). No significant difference was observed between groups (normal saline vs. iopamidol, 0.97 ± 1.08 vs. 1.04 ± 0.88, P = 0.79; normal saline vs. lipiodol, 0.97 ± 1.08 vs. 1.10 ± 0.80, P = 0.59; iopamidol vs. lipiodol, 1.04 ± 0.88 vs. 1.10 ± 0.80, P = 0.77).
Changes of acute inflammation, chronic inflammation, and fibrosis at each time point
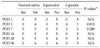
Table 1 summarizes the results of acute, chronic inflammatory response, and fibrosis at POD 1, 3, 7, 14, 28, 56 after injection of contrast agent and normal saline. There are no significant differences at each point after injection of normal saline and iopamidol. However, acute inflammatory response of POD 14 in lipiodol group was significantly higher than POD 28 and POD 56 using ANOVA and Tukey post hoc analysis. Similarly, in lipiodol group, chronic inflammatory response at POD 28 was significantly higher than POD 1, POD 3, POD 7 and POD 14 in ANOVA and Tukey post hoc analysis. Fibrosis of normal saline injection after POD 14 and iopamidol injection after POD 7 was significantly higher than POD 1and POD 3 in normal saline group and POD 1 in iopamidol group using ANOVA and Tukey post hoc analysis. However, there are no differences between all periods in lipiodol group using ANOVA and Tukey post hoc analysis.
Fibrinoid necrosis
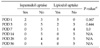
The presence of acute fibrinoid necrosis was observed in each group on POD 1, 3, 7, but did not show the difference between groups (Table 2).
Mesothelial hyperplasia
There was no significant difference in mesothelial hyperplasia at each time points between groups (Table 3).
DISCUSSION
Surgeons frequently express concerns about complications from gastric cancer surgery in patients receiving large area lymph node dissection. Location of lymph node metastasis from gastric cancer is reported to be distributed widely as a result of the complicated perigastric lymphatic network. Generally, when the depth of invasion confined to mucosa in early gastric cancer, the rate of lymph node metastasis have been reported as 1 to 3%, and submucosa as 11 to 20% [17-19]. However, because preoperative diagnostic techniques, including CT and endoscopic ultrasonography, do not provide an accurate prediction of metastasis in the regional lymph nodes, gastrectomy with extensive lymphadenectomy (D2 or D2 + a) is still considered as a standard surgical treatment for early gastric cancer in some centers [20]. In addition to prolonged operation time and hospital stay, the operative complications accompanying extended lymphadenectomy, such as leakage of anastomosis, bleeding, pancreatitis, intra-abdominal abscess, leakage of lymphatics cannot be trivialized [21,22]. Therefore, limited surgery such as laparoscopic wedge resection with limited regional lymph node dissection was attempted by Ohgami et al. [23] to overcome the complication and improve the quality of life in patients with early gastric cancer.
There are several methods of detecting the sentinel node. However, it is more difficult to detect the sentinel node in gastric cancer, because the lymphatic drainage of the stomach is considerably more complex than that of ectodermal organs like breast and skin due to the complex embryological development. Although it has been considerable debate on the advantages and disadvantages of different detection methods, a growing number of investigators used radiocolloid or a combination of both methods in more recent studies [24,25]. However, this method has the disadvantage of impossibility of predicting the accurate locations of primary sentinel nodes preoperatively because of the limited spatial images and the lack of distinct anatomy of the surrounding structures. Another problem which may occur are that use of radioisotope needs a special facilities, detection of correct sentinel node needs an experience and a technical learning curve, and the detection of radioactive lymph nodes adjacent to the injection site is difficult because of the shine-through effect.
Although there is insufficient evidence for applying CT lymphography to gastric cancer, recent studies have shown that CT lymphography can be an alternative SLN navigation surgery method for esophageal cancer [26]. In that study, they identified SLNs with 100% sensitivity by CT lymphography. However, another study of CT lymphography for gastric cancer reported only a 30% detection rate. Not only the technical aspects of CT lymphography, but also the tumor characteristics are important factors for achieving a higher rate of SLN detection in gastrointestinal cancers.
A technique using interstitial CT lymphography with the widely available iodine contrast medium such as iopamidol or lipiodol is an alternative method for preoperative sentinel node mapping and biopsy examination with a scintigraphic method [14,27,28]. Suga et al. [28] showed an interstitial CT lymphography with endoscopic mucosal injection of iopamidol was applicable for sentinel node navigation of superficial esophageal cancer. In this manner, it may be useful for planning the operative field and limited lymph node dissection, and for avoiding unnecessary extended lymph node dissection if surgeons identify the preoperative visualization of lymphatic spread and sentinel node draining from the primary cancer on CT lymphography. However, there is a limitation of application of this method to clinical practice, because tissue reactions after injection of iodinated contrast media have not been reported recently.
Our experimental investigation was performed to evaluate the response of gastric wall histology to direct effects of iopamidol or lipiodol. The degree of safety in using a contrast media needs to be determined before intelligent contrast media choices can be made. Our study demonstrated a lesser pathological response with iopamidol than lipiodol. We presume that this may be due to the water-soluble characteristics and relatively rapid wash-out nature of iopamidol. However, we did confirm that appearance of foreign body reaction, such as foam cell, after injection of lipiodol can make confuse the diagnosis of signet ring cell carcinoma.
A frozen section examination of the proximal cut-end adjacent to the lesion is an important step during gastrectomy. Previous reports have demonstrated that a positive margin is associated with a worse outcome [29-31]. Injection of contrast media into specimens for CT lymphography can cause a tissue reaction, including acute and chronic inflammation and a foreign body reaction. This process can create confusion when performing frozen and routine pathological examinations. These findings prompted us to investigate the histological reactions after injection of contrast media during CT lymphography.
Another purpose of this study was to determine how long contrast media can remain in tissue. We examined high-resolution X-rays using mammography after injecting contrast media. As a result, we found that lipiodol remained in the tissue much longer than iopamidol.
Because we only focused on the feasibility of using contrast media during CT lymphography, we cannot validate the clinical feasibility of CT lymphography. We only found potential difficulties with contrast media during CT lymphography. Further study including SLN mapping techniques is needed to show clinical feasibility and to provide the clinical significance of SLN detection using CT lymphography.
In conclusion, we conclude that iopamidol and lipiodol when used as a contrast media of CT lymphography is an available material of preoperative sentinel node navigation surgery for gastric cancer with a acceptable incidence of pathological alterations in an mouse model, and our results are potentially useful to clinical (human) application.
However, these agents can produce an acute inflammatory reaction within 7 days after injection. In particular, there is a possibility of causing a foreign body reaction after lipiodol injection from POD 3.







 XML Download
XML Download