

 ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The incidence of diabetes has been increasing globally at an alarming rate. The World Health Organization currently estimates that type 2 diabetes mellitus (T2DM) affects 171 million people worldwide. With an increase in the number of obese children diagnosed with T2DM, it is predicted that more than 366 million people will be affected by diabetes by year 2025 [1]. Such a rapid increase in diabetes is thought to be related to economic growth, westernization of life style, reduction of physical activity, emotional and physical stress and the extension of life expectancy. Although current antidiabetic treatment includes a variety of medications with enhanced efficacy, T2DM and the associated complications remain a substantial burden on the affected individuals and the society as a whole.
T2DM is characterized by resistance to insulin signaling, and is closely associated with obesity. The normal metabolic, neural and hormonal effects of the small intestine on the pancreatic islets, referred as the enteroinsular axis, are altered in patients with T2DM. When T2DM is associated with morbid obesity, weight loss induced by bariatric surgical procedures has been shown to be extremely effective in improving or resolving diabetes [2-4]. Increased insulin sensitivity accompanying the weight loss appears to be the most likely explanation for the improvement in diabetes in these patients. However, improvement from diabetes following the procedures that bypass the foregut (i.e., stomach, duodenum, proximal jejunum) such as gastric bypass or biliopancreatic diversion (BPD) seems to occur almost immediately after the surgery, well before significant weight loss occurs [4], thus, suggesting additional mechanisms contributing to the rapid glycemic control. Gastric bypass has been shown to increase glucagon like peptide-1 (GLP-1) and peptide YY (PYY) secretion [5,6] and decrease ghrelin level [7]. It is speculated that the "pro-incretin" effects of gastric bypass is related to the anatomical exclusion of the foregut from the nutrient passage.
Amelioration of diabetes in patients undergoing subtotal gastrectomy with Roux-en-Y (RY) reconstruction was reported in 1955 [8]. When the duodenum of a lean diabetic rat is bypassed surgically, normal glycemic control is restored [9]. These reports collectively suggest a glycemic control mechanism present in the foregut, and the exclusion of this area from the nutrient passage may help improve insulin sensitivity and diabetes. Several hypothesis have been proposed to explain the change of glycemic control after foregut bypass; foregut hypothesis, hindgut hypothesis, anti-incretin hypothesis, etc.
Gastrectomy removes some portions of the stomach, and is indicated mostly in patients with gastric cancer and intractable ulcer disease. The gastrointestinal (GI) tract is reconstructed either by Billroth-I (B-I) or Billroth-II (B-II). While B-I gastrectomy preserves normal GI tract configuration, B-II gastrectomy limits food entrance into the duodenum. Based on the studies demonstrating a positive impact on diabetes through exclusion of the foregut, a diabetic patient undergoing B-II gastrectomy is suggested to improve from diabetes better than a B-I gastrectomy patient. It has not been shown, however, in a systematic way whether duodenal exclusion by B-II reconstruction improves diabetes when compared to B-I gastrectomy. Because of a high incidence of gastric cancer in Korea, a significant number of gastrectomies are performed annually. The aim of this study is to examine retrospectively and compare the progression of diabetes in non-obese patients undergoing gastrectomy.
METHODS
Patients
From June 1996 to September 2009, a total of 2,134 Korean patients with stomach cancer underwent radical gastrectomy at Inha University Hospital (1,433 radical subtotal gastrectomies, 701 radical total gastrectomies). T2DM was noted in 169 patients (T2DM prevalence rate, 7.9%). Diagnosis of T2DM was based on fasting blood glucose (FBG) concentrations according to criteria established by the American Diabetes Association [10]. In addition, patients with a known history of T2DM and using diabetic medication prior to surgery were also classified as having T2DM regardless of FBG or glycosylated hemoglobin A1c (HbA1c) levels. Cancer of the stomach was established by endoscopic biopsy in all cases. Three patients who had undergone intestinal resection due to other diseases, six patients who had pancreatectomy due to gastric cancer invasion, one patient with body mass index (BMI) greater than 30, five patients with other endocrinopathies were excluded from the study. Five patients expired within 6 months after operation, and 28 patients who died prior to the study were also excluded from the analysis. From the total of 121 patients during this period, 75 of these patients were evaluated for follow-up (62.0%). Clinical data collected for this study include age, sex, onset of DM, duration of DM, pre- and postoperative FBG, BMI, serum HbA1c, diabetic medications, serum lipid levels. The study protocol was approved by the Institutional Review Board of Inha University Hospital (no. 08-115).
Operative method
Because all patients had stomach cancer, radical oncologic resection of stomach was performed. Radical oncologic gastric resection includes omentectomy, D2+α lymph node dissection, and required negative resection margin in all cases. The operation methods carried out were the radical total gastrectomy and RY esophagojejunostomy, radical subtotal gastrectomy B-I and radical subtotal gastrectomy B-II, with the operation chosen by location of cancer and operator's decision regardless of patient's diabetes status. In subtotal gastrectomy, approximately 75% of distal stomach was resected and intestinal continuity was maintained by B-I or B-II reconstruction. In cases of close proximity of cancer to the pylorus, supra-and infrapyloric lymph node invasion, and excessive tension for B-I reconstruction, B-II reconstruction was performed for intestinal continuity with 15 to 20 cm of afferent limb. In total gastrectomy, RY esophagojejunostomy was performed with 40 cm Roux limb and 20 cm afferent limb. And in all patients, vagotomy was routinely performed with the course of lymph node dissection.
Analytical methods
The established guidelines for determining diabetes resolution and improvement were followed. The parameters monitored for this included the changes in medication requirements, fasting blood sugar (FBS) and HbA1c levels. Based on the changes in medication requirements, FBS and HbA1c levels, each patient's postoperative diabetes status was divided into resolved (degree 1, no medication, normal FBG and HbA1c < 6.0%), diet-controlled (degree 2, no medications, 7% > HbA1c > 6%, FBG > 125 mg/dL), improved (degree 3, fewer medications or normal FBG and HbA1c decrease > 10% on same dose), unchanged (degree 4, unchanged medications and biochemical markers) or worsened (degree 5, more medications or increased FBG and HbA1c > 10% on same dose). Additional pre- and postoperative clinical factors such as age, sex, onset of DM, duration of DM, pre- and postoperative FBG, BMI, serum HbA1c, diabetic medications, serum lipid levels were compared and analyzed according to diabetes status.
Statistical analysis
All pre- and postoperative clinical indices were analyzed by Fisher's exact test. And the results of frequency across the three operation groups were analyzed by analysis of variance. The proportion of weight loss and other biochemical markers was also calculated for each patient and compared to their change in diabetic status. Finally, multivariate analysis according to operative method adjusting other clinical factors was performed with logistic regression test. All statistical analysis was carried out using SPSS ver. 15 (SPSS Inc., Chicago, IL, USA). Results were considered statistically significant if P < 0.05.
RESULTS
Clinical characteristics of patients (Table 1)
Preoperative demographics, diabetes related biochemical data for the total study population are listed in Tables 1. Fifty-four men and 21 women were included in the study (gender ratio, 2.6:1). The preoperative mean BMI was 23.8 ± 2.9 kg/m2 (range, 15.6 to 29.9 kg/m2) and mean HbA1c was 7.4 ± 1.6% (range, 4.8 to 12.2%). When stratified by the duration of DM, 33 patients (44%) had DM for less than 5 years, 18 patients (24%) for 5 to 10 years, and 24 patients (32%) had the diagnosis of DM for in excess of 10 years. Nine patients (12%) had diet-controlled DM with no medications. While 51 patients (68%) were on oral hypoglycemics, 15 patients (20%) were noted to be insulin user. The diet control patients are included more in B-II and RY group. Higher percentage of the RY esophagojejunostomy patients were on oral agents than insulin when compared to the B-I or B-II patients (P = 0.022). There were no significant differences of the other clinical parameters between the groups except severity of DM.
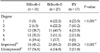
The change of clinical factors after gastrectomy (Table 2)
The changes in the clinical indices (BMI, FBG, HbA1c, cholesterol levels) following gastrectomy were listed in Table 2. There was no difference in the duration of follow-up periods (B-I, 35 months; B-II, 38 months; RY esophagojejunostomy, 32 months). The decrease in BMI after RY esophagojejunostomy is 11.7% and this is statistically greater compared to the weight loss resulting from the other operative methods. No other changes in the clinical indices were statistically significant.
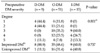
Factors associated with postoperative DM improvement (Table 3)
The factors associated with DM improvement were analyzed. The patients were stratified into two groups: those with improvements from preoperative DM vs. those with no improvements or worsening. When the patients DM duration was less than 5 years, improvement of DM was seen in 50% (26 patients). When the duration of DM was longer (more than 5 years), fewer number of patients achieved improvements from DM (15.4% and 34.6% for 5 to 10 years and over 10 years groups respectively). No changes or worsening of DM status were seen in 7 cases (30.4%), 10 cases (43.5), 6 cases (26%) respectively according to the same period, and these values showed statistical significance (P = 0.036). Reconstruction method has statistical significance between the improved and the unimproved (P < 0.001), and this is the most powerful factor showing the difference between the two groups. There was no correlation between other preoperative clinical factors and the postoperative changes in diabetic status.
Procedure specific improvement of DM (Table 4)
The status of DM was studied before and after each specific procedure type. The degree of DM improvement was classified into five subgroups based on changes in FBS, HbA1c and medication requirements. No resolution of diabetes was noted in B-I patients. 45.2% of the B-I patients improved while DM of 54.8% of patients were unchanged or worsened. Contrast to B-I group, the resolution rate of B-II and RY esophagojejunostomy group was 22.5% and 23.5% respectively, and 85.2% and 88.2% of patients showed improvements respectively (P < 0.001). When duodenal bypass group (B-II and RY) was compared collectively to the B-I patients significantly increased resolution of DM (22.7%) and improvement (86.3%) were seen in the duodenal bypass group.
Preoperative DM severity and postoperative improvement in DM status (Table 5)
Patients requiring insulin preoperatively showed no resolution of DM postoperatively. Only 60.0% of the insulin users showed postoperative improvements; however, non insulin user showed 16.7% resolution and overall 71.7% of improvement rates (P = 0.001).
Multivariate analysis of procedure-specific improvements in DM (Table 6)
The postoperative changes in DM status following specific procedure (B-I, B-II, RY esophagojejunostomy) were compared by adjusting other clinical factors which may affect diabetes control such as age, sex, DM duration, severity, basal HbA1c and ΔBMI. The improvement rate of DM status was 7.46 and 7.87 times higher in B-II and RY esophagojejunostomy group respectively, than that in B-I group (Table 6). I would like to emphasize this result; B-II caused 7.46 fold improvement of T2DM although B-I and B-II resulted in similar weight loss. It should be explained.
DISCUSSION
T2DM affects a large population of patient across the world, and despite newer class of medications, it is a progressive disease leading to microvascular complications [11]. Although tight control of blood sugar may delay progression of the disease, an increased requirement of medications over time is commonly seen despite modest weight loss by diet and exercise even in patients with BMI less than 30 [12]. Morbidly obese patients with T2DM are noted to improve in their diabetes following successful weight loss surgery [13]. Weight loss achieved by these procedures is commonly believed to be the primary mechanism of improved insulin sensitivity, ultimately leading to improvement in T2DM. Our current data show that gastrectomy patients achieve significant improvement and/or resolution of T2DM. Furthermore B-II showed 7.46 times higher rate of improvement of T2D than B-I which lost similar body weight. The mechanism of improvement in T2DM in our study patients, thus, cannot be explained by simple weight loss.
Some of the bariatric procedures seem to achieve more profound improvement in T2DM than others. For example, BPD has been shown to have a marked and sustained improvement in diabetes with 95 to 100% patients achieving resolution [14,15]. Similarly, gastric bypass induces resolution of diabetes in 83 to 85% patients in the long term [12,13,16]. In contrast to such bypass operations, purely restrictive bariatric procedures without alterations in intestinal continuity (i.e., vertical banded gastroplasty or gastric banding) achieve weight loss by limiting caloric intake by reducing the size of the functional stomach. Improvement of T2DM following these procedures; however, seem to take a longer time and is far less than that seen in their bypass counterparts. The non-obese gastrectomy patients with duodenal bypass in this study (B-II and RY esophagojejunostomy) clearly improve more dramatically from T2DM when compared to B-I patients who continue to have passage of nutrients through the duodenum. Our data is thus consistent with the observation of enhanced DM improvements in obese patients undergoing the bariatric procedures with proximal small intestinal bypass. These findings suggest an additional mechanism(s) of glycemic control located in the proximal small bowel independent of weight changes.
Bypass of the proximal small intestine in bariatric procedures appears to cause profound postoperative alteration in the secretion of GI peptides that affect insulin secretion and insulin sensitivities. Examples of these peptides include GLP-1, gastric inhibitory polypeptide (GIP) and PYY [17]. GLP-1, which is produced by L-cell in colon and ileum, induces proliferation of beta cells and promotes insulin secretion in pancreas, and its secretion is increased after gastric bypass surgery [18]. More rapid delivery of nutrients to the distal intestine due to the bypass anatomy is thought to be responsible for the enhanced GLP-1 secretion. Ghrelin, unlike GLP-1, decreases pancreatic insulin secretion while increasing food intake and GI motility. Ghrelin levels are known to decrease after gastrectomy or gastric bypass [7], may be contributing to the improvements of T2DM in our gastrectomy patients. The changes in ghrelin and GLP-1 levels were not measured in this retrospective study. All patients in this study underwent radical gastrectomy which includes turncal vagotomy and omentectomy, both of which may also be contributing to the improvement in diabetes in our patients.
Gastric cancer is one of the most prevalent cancers in Korea and Japan, and radical gastric resection is one of the most common types of surgery performed in East Asia. The preferred type of reconstruction following gastrectomy is a controversial subject. B-I anastomosis is considered the most physiologic reconstructive procedure, and it is the procedure of choice in distal gastric cancer patients. Based on our results of dramatic improvement in DM following duodenal bypass anatomy (7.46 fold improvement over B-I reconstruction), perhaps B-II or RY reconstruction should be considered in diabetic gastric cancer patients.
Most of the data in post-surgical T2DM improvement come from morbidly obese patients undergoing weight loss surgery even in Korea [19,20]. Less obese patients (BMI < 35) with T2DM also seem to improve from diabetes after gastric bypass [21]. Our study shows significant improvement and/or resolution of T2DM is also achieved in patients who are not obese. The resolution rate of T2DM in non-obese Korean gastrectomy patients from this study seems somewhat lower than that seen in morbidly obese patients after bariatric surgery. T2DM in Korean patients is characterized by deterioration of early-phase insulin secretion [22]. Therefore, T2DM in Korean patients appears to be associated with a severely impaired β-cell function, thus less likely to reverse compared to early insulin resistance without significant beta-cell dysfunction seen in the Westerners [23]. Nevertheless, marked improvements in T2DM are seen our non-obese patients, particularly when the reconstruction is performed with duodenal bypass anatomy. Although tight glycemic control with medication (HbA1c less than 7%) has been shown to decrease the risk of microvascular complications associated with diabetes [24,25], such tight control with medication is difficult to achieve. Currently, no GI surgical procedure is approved to treat T2DM in non-obese patients. This is particularly important in East Asian countries where an alarming increase of T2DM is seen in patients who are non-obese but exhibit centrally obese anthropometry associated more with insulin secretory defects than insulin resistance [26]. The current data suggest the potential for effective surgical treatment for such non-obese T2DM patients.
There was no correlation between preoperative clinical factors with postoperative changes in diabetes status. The duration of preoperative T2DM and the duodenal bypass surgical anatomy were identified as the only significant factors that affect the postoperative diabetic status. Shorter preoperative DM duration appears to predict better improvement in DM postoperatively. In addition, complete resolution was not seen in insulin using patients, and only 60% of these patients achieved improvement. In contrast, 16.7% of the oral hypoglycemics users were able to achieve complete resolution along with additional 20.0% coming off all hypoglycemics, totally an overall improvement rate of 71.7%. Regardless of the type of reconstruction, improvement from DM was less prominent in insulin using patients. These patients are likely to be hypoinsulinemic as well as insulin resistant. The remaining pancreatic β-cell function may be an important determinant of the likelihood of T2DM resolution following gastric surgery [27]. Based on these, it appears that β-cell deterioration might be reversible at least early in the course of the disease and that it is best to intervene before permanent islet cell injuries occur.
There are several limitations in our study. In this retrospective study, some of the important biochemical parameters could have been studied pre- and postoperative periods. These include levels of GLP-1, ghrelin, PYY and other pertinent diabetic markers. Formal oral glucose tolerance tests would have also strengthened this study. The patient follow-up was not established regularly as a prospective study, and thus, the data points are not precisely matched. The criteria of the improvement is arbitrary although the criteria of the resolution matched the criteria of American Diabetes Association. That caused high rate of the improvement after surgery, comparing with other reports [28,29]. Radical gastrectomy and reconstruction is quite different from the procedure employed in metabolic surgery (remaining stomach, long afferent limb etc.) The outcomes can be affected by many factors, such as disease stage, type of resection, extent of surgery, adjuvant treatment, or postoperative weight change. Especially, the degree of weight loss would be the most important factor which associated with control of diabetes. But my institute has two special surgeons for gastric cancer surgery, and they operated all patients enrolled. So the extent and type of operation can be consider as a standard method in general without any intention because there was no idea of metabolic surgery at the time of the operation. As for the influence of adjuvant chemotherapy, the patients may be considered as the recovered because the recent patient was enrolled at 2 year after the surgery.
To improve the shortcomings of the current retrospective study, a prospective randomized study is being initiated with a regular long term follow-up protocol, collection of more comprehensive data elements including all known incretins, diabetes markers, gut hormone levels.
Lastly, this paper has limited worth just to give a glimpse into the possibility of metabolic surgery although it does not have any datum of entroinsular physiology. Till now, T2DM is a progressive and dreadful disease, but it is notable finding that some surgical procedures can improve the T2DM even in non-obese patients. Especially, we should take notice B-II showed 7.46 times higher rate of improvement than B-I which induced weight loss similar to B-II.
In summary, bypass of the foregut seems to have some mechanism of glycemic control beyond weight loss, which may mean that metabolic surgery can be a candidate to control T2DM.




 XML Download
XML Download