

 ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Dendritic cells are arachnoid immune accessory cells originating on hematopoietic stem cells, and sarcoma on dendritic cells is divided into various subtypes including Langerhans cell sarcoma, interdigitating dendritic cell sarcoma (IDCS), follicular dendritic cell sarcoma, dermal dendrocyte sarcoma, interstitial dendritic cell sarcoma and veiled cell sarcoma [1]. Most IDCS occurs in the lymph node (particularly in the collum, the mediastinum and axilla) and around one third of it is found in other organs except the lymph node. For the organs, the liver is observed most frequently, while others are the spleen, the skin, the lung, the rhinopharynx, the small intestine and the breast [1,2].
The incidence rate of IDCS was reported to be slightly higher in males than in females (1:1.4), and its mean age at onset was about 46 years but it was shown in all age groups (14 to 80 years) [3]. Its prognosis is highly aggressive.
Against this background, a case diagnosed as IDCS of the axilla and treated in Soonchunhyang University Hospital is reported.
CASE REPORT
A 57-year-old female visited Soonchunhyang University Hospital with a left axillary mass palpated for the last two months as a chief complaint. The first physical examination found no specific abnormality such as pain or burning sensation except the palpable mass in the left axilla. The mass was hard and fixed.
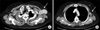
Chest computed tomography (CT) showed an approximately 7 cm mass clearly observed in the left axillary region and several lymph nodes enlarged to be 2 cm around the mass (Fig. 1).
Breast ultrosonography and mammography were performed first to determine whether it was breast cancer or not but revealed no mass in the breast and no calcification lesion, respectively. Next, core biopsy found an abnormality suspected to be sarcoma in the lymph node, so additional tests were conducted to check its primary site.
Colonoscopy and gastroscopy revealed no abnormality and abdomen CT also did not reveal a primary site. Bone marrow biopsy to examine bone marrow involvement recorded a negative result. Lastly, positron emission tomography (PET) CT also found no specific abnormality except the increase of 18-fluoro-deoxyglucose in the left axillary region (Fig. 2).
The patient underwent left axillary lymph node dissection (level I, II) as she was thought to have sarcoma originating in the axillary lymph node. Permanent pathologic report finally diagnosed it as IDCS originating in the axillary lymph node (Fig. 3). The microscopy showed ill-defined, paracortically proliferating irregular nests of spindle to ovoid cells in fascicles. The remaining follicles were frequently seen. The tumor cells showed mild to moderate nuclear atypia. Mitosis was rarely seen and necrosis was not present. Immunohistochemistry showed that S-100 protein, vimentin, CD99, CD68 and cyclin D1 were positive and CD34, CD20, CD21, CD23, CD3, HMB-45, desmin and melanin A were negative. Ki-67 or a tumor marker was around 10%.
After the surgery, the patient was treated only with radiotherapy not chemotherapy as adjuvant therapy and recurrence has not been observed for thirteen months up to now.
DISCUSSION
Interdigitating dendritic cells are an antigen presenting cells observed on T cells of the peripheral lymphoid tissues, and sarcoma originating on it is very rare and is histologically similar with B cell lymphoma or T cell lymphoma and other spindle cell neoplasm [2].
Due to this similarity, it is hard to distinguish through hematoxylin and eosin staining, which is conducted frequently for pathologic diagnoses [1]. So, immunohistochemistry is necessary to confirm IDCS. For the sarcoma, S-100 and CD45RB protein, HLA-DR and vimentin are positive and CD1a, CD21, and CD35 protein are negative while CD68 is positive or negative. Another property in differentiating it is its structural characteristics. It has been reported that interdigitating cytoplasmic processes or one characteristic of interdigitating dendritic cells existed on the surface of cells but Birbeck granules were insufficient [4]. There is no biomarker specific only to IDCS [2].
However, despite these characteristics, it is very hard to distinguish it from malignant melanoma because malignant tumors also show a positive result in S-100 protein and CD68. So, IDCS cannot be diagnosed only with the results of immunohistochemistry and should be done by considering clinical results of all examinations [2].
In this study, the postoperative pathologic report recorded that S-100 protein, CD68 and vimentin were positive while CD21 and melanin A were negative. But, the possibility of metastatic melanoma could not be excluded completely. Thus, visual inspection of the total skin, abdomen CT, gastroscopy, colonoscopy and PET CT were conducted finding no possibility of melanoma.
IDCS does not generally provoke any specific symptom. Its symptoms are similar with those of lymphadenitis and can include fever and constitutional symptoms such as decreased body weight in some cases [2].
Although any guideline to treat IDCS has not been established as it is very rare, a surgical excision is primarily applied because its lesion is limited to the site of origin in most cases [1-4].
As adjuvant therapy after the surgery, chemotherapy and radiotherapy can be considered. Kairouz et al. [5] insisted that postoperative radiotherapy increased disease free survival, but it has not been accepted as a standard treatment.
Chemotherapy also was reported to be effective in some studies, but it was not accepted as an infallible therapy.
Efune et al. [6] showed that ABVD (adriamycin, bleomycin, vinblastine, dacarbazine) achieved complete remission. However, Olnes et al. [7] insisted that a good prognosis could be obtained only with ABVD chemotherapy without surgical treatment. But, De Pas et al. [4] found through literature review that many cases of IDCS were treated only with surgery even though its recurrence rate was actually 40% and the rate was not significantly different from the recurrence rate (32.6%) after adding chemotherapy and radiotherapy to the surgical treatment, so the adjuvant therapy did not reduce the recurrence.
Although large scale studies are necessary to prove its effect, verifying the effect is considered not to be easy due to realistic difficulties.
In Korea, IDCS in the tonsil and in the pleura was reported. While IDCS in the tonsil led to nearly complete remission after four time CHOP (cyclophosphamide, doxorubicin, vincristine, prednisolone) chemotherapy [8], the patient with IDCS in the pleura died in three months despite two time CHOP and one time IMEP (ifosfamide, methotrexate, etoposide, prednisolone) [9].
In Soonchunhyang University Hospital, postoperative chemotherapy for IDCS was not performed and the patient in this case has been followed up after radiotherapy. There has been no evidence of recurrence for thirteen months until now and she is followed up regularly.
For the course after treatment, as mentioned before, IDCS is very aggressive and metastasis at diagnosis is found more frequently than follicular dendritic cell sarcoma, so its prognosis is known to be very aggressive [4].
According to previous reports, average survival time is around nine months after postoperative chemotherapy and radiotherapy and survival of over five years is quite rare [2].
One of the factors affecting its prognosis was found to be the size of the sarcoma. Over 5 cm IDCS recorded a significantly higher recurrence rate than smaller ones (50% vs. 11%). Therefore, its size is considered to be very critical. Except that, mitotic count and necrosis were also reported to influence its prognosis. In addition, the authors of the report suggested that higher expression rate of Ki-67 could produce a negative effect on the prognosis but that needs to be studied more [4].
In conclusion, IDCS is a very rare sarcoma that is hard to diagnose and progresses fast; treating it is very difficult. Therefore, a proper treatment guideline can be established after more experiences and treatments are accumulated.


 XML Download
XML Download