

 ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Since the first performance by Kitano et al. [1], the use of laparoscopy-assisted distal gastrectomy (LADG) for early gastric cancer (EGC) in Korea and Japan has exploded because of the high prevalence of EGC and the merits of LADG, including less post-operative pain, earlier recovery and better cosmetic outcomes, over open gastrectomy [2-4]. Following laparoscopic distal gastrectomy (LDG), there are three major reconstructive methods, the Billroth-I, Billroth-II and Roux-en-Y, that can be used, and several studies have reported their safety and efficacy [5-7]. In Korea and Japan, Billroth-I is the most common reconstructive modality because of the maintenance of the physiological passage of food. Roux-en-Y reconstruction, which has a low incidence for bile reflux, has also been employed by some centers [5,7-10]. However, these reconstructive modalities have some problems, such as bile reflux, food stasis and complexity [11-13]. For this reason, Billroth-II reconstruction has commonly been performed after LDG because of its simplicity and the low rate of gastric stasis [13]. Although laparoscopy provides a wider surgical field than mini-laparotomy, in general, most surgeons have chosen mini-laparotomy at the upper abdomen for reconstruction because of the technical complexity of LDG and an unfamiliarity with intra-corporeal anastomosis. As surgeon experience in performing LDG has increased and improvements in laparoscopic instruments have been accomplished, for example, the development of the endoscopic linear stapler, totally laparoscopic distal gastrectomy (TLDG), including several intra-corporeal anastomotic techniques, has been introduced and its usefulness reported [5,9,14,15]. However, these reports have been mainly restricted to the Billroth-I and Roux-en-Y for reconstruction. In this study, we evaluated the safety and short-term outcomes of TLDG with reverse T-shaped intra-corporeal Billroth-II anastomosis using linear staplers.
METHODS
Patients
A total of 399 patients underwent LDG with Billroth-II reconstruction for gastric cancer between April 2004 and March 2011. During this period, patients were divided into two groups according to reconstructive method, such as intra-corporeal or extra-corporeal reconstruction. From April 2004 to September 2009, we performed extra-corporeal Billroth-II reconstruction on 269 gastric cancer patients (LADG group), and intra-corporeal Billroth-II reconstruction was applied to 130 patients (TLDG group) from October 2009 to March 2011. The selection for reconstructive method was based simply on the timing of operation. In the earlier period, we performed extra-corporeal anastomosis after LDG because of our unfamiliarity and lack of experience with intra-corporeal anastomotic procedures. As our experience with diverse intra-corporeal anastomotic with laparoscopic sewing and linear staplers accumulated, we were able to applied this technique to LDG. There was no difference between groups in perioperative and post-operative care. The patients resumed oral intake 2 to 3 days after surgery and were discharged 7 to 10 days after surgery. All patients received a continuous venous infusion of fentanyl for 2 days after surgery, and additional analgesics (one vial of ketorolac tromethamine) were injected intramuscularly if the patient complained of pain. The parameters for assessments were defined as follows. Morbidities related to anastomosis were leakage at the gastrojejunostomy and duodenal stump, bleeding at gastrojejunostomy site, gastric stasis and afferent loop syndrome. The run-time in anastomosis was from the extension of the epigastric trocar site to the completion of gastrojejunostomy in LADG and from resection of the stomach and retrieval of specimen to the perfection of gastrojejunostomy in TLDG.
Surgical procedure
All patients were placed in the supine position and subjected to a 15 to 20° reverse Trendelenberg position. An initial 10-mm trocar for a 30° flexible electrolaparoscope was inserted through the infraumbilical area using a Hassan technique. After establishing a pneumoperitoneum with carbon dioxide (CO2), the operator stood on the right side of the patient, and the CO2 pneumoperitoneum was maintained at 12 to 15 mmHg during the operation. The extent of resection was determined by the location of the primary tumor and lymph node status. Using ultrasonic-activated scissors (laparoscopic coagulation shears [LCS]; Ethicon Endo-Surgery Inc., Cincinnati, OH, USA), partial omentectomy with D1+β lymphadenectomy was performed mainly for EGC, but total omentectomy with D2 lymphadenectomy was performed in patients with advanced gastric cancer according to lymph node classification by the Japanese Gastric Cancer Association [16]. The duodenum was transected about 2 cm distal from the pylorus using a 45-mm endoscopic linear stapling device following the dissection of lymph nodes numbers 5 and 6. When an EGC was located mid-body, preoperative tumor localization using an endoscopic metallic clip (HX-600-090L, Olympus Co., Tokyo, Japan) was performed, and the identification of the tumor in LADG was performed by palpation of the metallic clip. The topographic location of the tumor was identified by intra-operative portable abdominal radiograph in TLDG. Following these procedures, distal gastrectomy and Billroth-II anastomosis was performed with a hand-sewing technique or using endoscopic stapling devices as described below.
Reconstruction in LADG
A total of 5 trocars were used in this procedure. Following establishment of pneumoperitoneum, two additional 12 mm and 5 mm trocars were introduced as main ports into the right side at 2 cm above the umbilicus and just below the costal margin, respectively. Then, a 10 mm trocar was inserted 4 cm below the xyphoid process for traction of the liver, and a 5 mm trocar was inserted in the left mid-clavicular line 2 cm above the umbilicus as an accessory port. After completion of lymphadectomy, a 10-mm trocar site at the epigastrium was extended approximately 5 to 6 cm vertically or transversely, and the distal part of the stomach was extra-corporeally resected with using a 100-mm linear stapling device. A segment of jejunum was adopted approximately 10 to 15 cm distal from Treitz's ligament, and hand-sewn extra-corporeal anastomosis was performed in an antecolic fashion between the remnant stomach and the jejunum with a continuous interlocking suture of 3-0 absorbable suture material and an overlying Lembert reinforcement via this window.
Reconstruction in TLDG
Initially, we used 5 trocars, but in the TLDG series, we reduced the number to 4 channels. Instead of a 10-mm trocar positioned at 4 cm below the xyphoid process for traction of the liver, liver retraction was accomplished by a retraction of the falciform ligament and the left lobe of the liver using a single suture on the mid-pars condensa of the lesser omentum. After distal gastrectomy was performed using one or two endoscopic liner stapling devices (Fig. 1A), the specimen was extracted via the vertically extended about 2- to 3-cm window of the 10-mm umbilical trocar site. The tumor free margin was examined. A double-ring wound retractor (Alexis, Applied Medical Resources Co., Rancho Santa Margarita, CA, USA) was inserted through the incision and rolled to cover the window. The device was comprised of a surgical glove, and one 10-mm trocar was latched onto the wound retractor ring, which was rolled over it to provide a seal. Following the re-establishment of the pneumoperitoneum, entry holes were made at both the greater curvature side of stomach and jejunum approximately 10 to 15 cm distal from Treitz's ligament using LCS (Fig. 1B, C). After the insertion of each arm of the endoscopic linear stapler into the remnant stomach and jejunum, vertical anastomosis along the greater curvature side of the remnant stomach was made by the firing of the endoscopic linear stapler via the 12-mm trocar site at the right abdomen (Fig. 1D). The common entry hole was horizontally or obliquely closed with one endoscopic linear stapler (Fig. 1E, F).
Statistical analysis
All statistical analyses were performed using the SPSS ver. 15.0 (SPSS Inc., Chicago, IL, USA). Pathological results were classified by 7th Union for International Cancer Control classification scheme. The two groups were compared using Student's t-test for continuous variables and are expressed as the mean ± SD. Categorical variables were analyzed using the chi-squares test. P < 0.05 was considered significant.
RESULTS
Patient characteristics
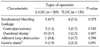
There was no conversion to an open procedure, and all procedures were completed under the given conditions. Demographics and clinicopathological characteristics are listed in Table 1. Of the 399 patients, 130 underwent TLDG, and 269 patients underwent LADG. There were no statistical differences between the two groups in clinicopathological features. EGCs were found in 92 (70.8%) and 172 (63.8%) patients out of the 130 and 269 patients, respectively, in the TLDG and LADG groups respectively. Mean tumor sizes and proximal resected margins were 3.1 ± 2.2 cm, 3.0 ± 2.2 cm and 4.3 ± 2.6 cm, 4.7 ± 2.7 cm, respectively. D1+β or D2 lymph node dissections were performed in most cases.
Surgical results and anastomosis-related complications
The outcomes of the operative procedures are listed in Table 2. The estimated blood loss was similar (131.0 mL vs. 150.0 mL) in both groups, but the mean operation and reconstruction times of TLDG were statistically shorter than LADG (212.5 ± 43.5 minutes vs. 226.1 ± 55.6 minutes, P = 0.019; 10.8 ± 3.9 minutes vs. 18.2 ± 6.6 minutes, P < 0.001). In addition, post-operative hospital stays of TLDG patients were shorter than LADG patients (8.3 ± 3.2 days vs. 9.9±5.3 days, respectively; P = 0.016), and the total number of parenteral analgesic administration in the LADG group was more frequent after surgery. However, there were no significant differences in the post-operative level of serum C-reactive protein and white blood cell count 1, 3 and 7 days after surgery.
Anastomosis-related complications were defined as follows. Anastomosis leakage was diagnosed by contrast leakage on plain radiography. Bleeding from anastomosis was detected by a Levin tube with transfusion or endoscopic therapy. Gastric stasis was not improved after fasting for 2 days and was eventually relieved by gastric lavage. Afferent loop obstruction, anastomotic leakage or bleeding, duodenal stump leakage and gastric stasis occurred in 11 (8.5%) TLDG and 21 (7.8%) LADG patients, and the incidence rate of these events was not significantly different between the two groups (P = 0.655) (Table 3). Of these events, duodenal stump leakage was the most common, followed by gastric stasis.
DISCUSSION
The major difference between LDG and conventional open distal gastrectomy is the length of the incision on the abdomen. Because of the smaller incision, LDG has advantages over open distal gastrectomy, such as early recovery with a less painful post-operative course and cosmetic efficacy. Most surgeons perform LADG, which consists of an appropriate systemic lymph node dissection and the mobilization of the stomach. LADG makes an approximately 5- to 6-cm long mini-laparotomy on the upper abdomen to perform extra-corporeal reconstruction. This reconstructive modality might lead to pain and increased injury from the forceful traction at the mini-laparotomy site. In our result, additional analgesics were required more frequently in the LADG group. In addition, extra-corporeal reconstruction via mini-laparotomy might be a complicated, stressful and time-consuming procedure. During extra-corporeal reconstruction, we performed hand-sewed anastomosis; however, extraction of the gastric remnant and jejunum via a narrow window was not easy and did not supply sufficient exposure of the lumens, especially in obese patients. We usually had a time restriction because the greater the length of time taken for an anastomosis, the greater the potential for congestion in the gastric remnant and jejunum, which might lead to anastomotic leakage. In contrast to the extra-corporeal procedure, intra-corporeal reconstruction offers a wider operative field than minilaparotomy and requires a shorter time because it is completed by the firing of the endoscopic linear staplers twice. In this study, the mean time for operation and anastomosis was significantly shorter than in the LADG group.
Our intra-corporeal Billroth-II reconstruction had some differences from conventional Billroth-II reconstruction, which was made between the end of the remnant stomach and the side of the jejunum. Anastomosis in intra-corporeal reconstruction was made at the posterior wall of the remnant stomach parallel to the greater curvature. The merits of this method were as follows. First, it was easy and safe to close the entry hole. During the enveloping of the entry hole, surgeons have generally positioned the endoscopic linear stapler vertical to the direction of the jejunum to prevent potential afferent loop narrowing or obstruction in the proximal jejunal limb. However, it was difficult to perform a vertical closure because of the difficulty in positioning the endoscopic linear stapler. In our procedure, the stapling line for closing the entry hole was oblique to the direction of the jejunum. Although this closure might have potential for afferent loop obstruction, no afferent loop obstruction or related symptoms were observed. One afferent loop obstruction was due to an internal herniation of the entire jejunal segment through the posterior space of the remnant stomach (Petersen hernia). Therefore, this modality was feasible and safe. Second, this procedure reduces the number of trocars. Generally, 5 to 6 trocars, including one or two 12-mm sizes, are used for the operation, and reconstruction is performed at either the right or left side of the patient. However, we used 4 trocars, and the reconstructive procedure was achieved on the right side of the patient without a change in the surgeon's position. This might also be related to the low dose of additional analgesics and the shorter post-operative stay in the TLDG group. Third, it was easy to examine and control the existence of bleeding from the anastomosis site. Bleeding from the stapled line occurred, and in this case, it was necessary to control it. If the entry side was located on the left side of the patient, it was hard to check the stapled line due to the limitation of the direction of the laparoscope.
There were no differences in anastomosis-related morbidities between groups. However, bleeding from the anastomosis site in the intra-corporeal procedure tended to be higher than the extra-corporeal method. With the endoscopic linear stapling device, immediate or delayed bleeding at the stapled line might occur, especially at the anastomosis site between the remnant stomach and jejunum. Four patients actually developed bleeding in the TLDG group in the earlier series. After this series, we examined the presence of bleeding focus by washing with normal saline, and we controlled bleeding with laparoscopic clips to prevent post-operative intra-luminal bleeding. There was one leakage from gastrojejunostomy in the intra-corporeal procedure, which was managed by percutaneous drainage. This rate was acceptable compared with other reports in with intra-corporeal and extra-corporeal reconstructions [13,17,18].
Although Billroth-I reconstruction was the typical choice after distal gastrectomy in Korea and Japan because of the preservation of the physiological passage and simple closure using staplers, about 40% of Korean surgeons performed Billroth-II reconstruction [19]. The merits of Billroth-II reconstruction compared to Billroth-I are a lower food stasis rate and a larger extent of resection. If the tumor is located in the middle third of the stomach, it is difficult to perform Billroth I reconstruction because excessive tension might develop at the anastomosis site if a safety margin was included. For this condition, Roux-en-Y reconstruction is recommended as an alternative method [7-10]. The advantages of Roux-en-Y reconstruction are low bile reflux and prevention of bile reflux, thus preventing gastritis and gastric cancer in the remnant stomach [7,20]. However, this procedure requires multiple anastomosis and involves a risk of Roux stasis. For food stasis, this procedure is stressful to both patients and surgeons, and most Korean surgeons have been reluctant to perform this procedure [6,19].
An accurate localization of the lesion and confirmation of the tumor-free margin are mandatory for oncological demand. The main concern for intra-corporeal anastomosis is how to determine the resection line for a sufficient proximal margin. During the extra-corporeal procedure, it was not difficult to confirm the resection line because it was possible to palpate the tumor or the clips that had been applied preoperatively. In the intra-corporeal procedure, although the preoperative endoscopic clipping was performed around the lesion, there was little tactile sensation for the lesion, and it was hard to confirm the resection line, especially for a tumor that was located at the middle part of the stomach. For this reason, various methods, such as endoscopic tattooing, intraoperative endoscopy, laparoscopic ultrasonographic localization and intraoperative fluoroscopy, have been introduced to localize the tumor [21-24]. We usually performed an intraoperative portable abdominal radiograph if EGC was located in the middle part of the stomach and a sufficient tumor-free proximal resection margin could be achieved. In the present study, there was no difference in the proximal resection margin.
In conclusion, our results demonstrated that intra-corporeal Billroth-II anastomosis is a feasible procedure that can be safely performed with the proper experience for LDG. This procedure may be less time consuming and may produce a more cosmetic result. However, surgeons should pay attention to prevent bleeding from the staple line, especially when performing intra-corporeal anastomosis using endoscopic linear staples. This study was retrospective and TLDG procedure was performed after many experiences in LADG. Therefore, there was a little limitation for comparing with absolute numerical value between two groups. Therefore, prospective study might be needed to confirm the feasibility and merits of TLDG.



 XML Download
XML Download