

 ePub
ePub Citation
Citation Print
Print


INTRODUCTION
A colon perforation is uncommon, and is usually caused by diverticulitis, trauma, malignancy, amoebic colitis, or ulcerative colitis [1]. Although rare, a stercoral ulcer could also cause colon perforation [2-7]. Stercoral perforation of the colon was first described by Berry [8] in 1894 . To date, fewer than 150 cases of stercoral perforation of the colon have been reported in English literature [9]. This report concerns a case of stercoral perforation of the descending colon that underwent re-operation for successful management.
CASE REPORT
A 69-year-old female was admitted to the department of surgery through the emergency room with a chief complaint of abdominal discomfort with a slip-and-fall injury. She had a 5-year history of Parkinson's disease and was treated at the out-patient clinic of this hospital with regular medications. She had undergone a radical total gastrectomy due to advanced stomach cancer 5 months prior to admission. She was taking a 5-cycle intravenous chemotherapy regimen for treatment of advanced stomach cancer. During chemotherapy treatment, she underwent total hip replacement (THR) of the right hip due to a hip fracture 1 month prior to admission. After the THR, she complained of constipation and had taken some kind of laxatives.
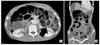
On physical examination in the emergency room, her body temperature was 36.8℃, heart rate was 112 per minute, blood pressure was 160/100 mmHg, and respiratory rate was 20 per minute. Abdomen was rigid at the left lower quadrant. Laboratory examination showed that white blood cell count was 7,510 cells/mm3 (segment form, 85.8%), as well as the following abnormal blood chemistry: albumin, 2.6 g/dL, sodium 130 mEq/L, and potassium 3.1 mEq/L. Other laboratory results were within normal range. Abdominopelvic computed tomography (CT) revealed a large amount of fecal impaction of the colon with colonic distension, and free intraperitoneal air with adjacent extraluminal air bubbles at the descending colon (Fig. 1). The initial clinical diagnosis was traumatic perforation of the descending colon. Emergency surgery was performed. Intraoperatively, there was an obvious perforation, approximately 1.0 cm in diameter, in the antimesenteric border of the descending colon just distal to the splenic flexure. On palpation of the colon, we found a significant amount of firm stool throughout the colon. Because the rim of the perforation site was clean, primary repair with diverting terminal ileostomy was performed. Postoperatively, she recovered well until postoperative day (POD) five. On the sixth POD, she complained of newly developed left upper quadrant pain. During wound dressing, dirty discharge was found. Therefore, we suspected re-perforation of the colon at the primary repair site. Repeated CT findings were the same as the previous CT findings. On examination, her body temperature was 36.7℃, heart rate was 112 per minute, blood pressure was 130/90 mmHg, and the respiratory rate was 20 per minute. Laboratory examination showed that white blood cell count was 8,040 cells/mm3 (segment form 90.8%). We decided on re-operation. We found that the primary repair site was perforated again and two fecalomas were found in the intraperitoneal space near the perforation site. Sigmoid colotomy was performed 20 cm distal to the primary perforation site. Through this colotomy, stool was removed digitally. After removal of all impacted stool, the colotomy site and primary perforated site were closed. After re-operation, she showed steady recovery with conservative treatment.
DISCUSSION
Stercoral perforation means "perforation of the large bowel due to pressure necrosis from a fecal mass" [6]. Stercoral perforation of the colon has been reported to be 3.2% of all colonic perforation [5] and the mortality rate of stercoral perforation was maximal at 35% in the literature [7]. Stercoral ulcers usually occur in debilitated, bed-ridden, mentally ill, or narcotic-dependent patients [4]. The most influential factor in development of a stercoral ulcer is chronic severe constipation. For our case, she was diagnosed with Parkinson's disease 5 years prior. A prevalence of constipation occurs in the range of 70 to 80% and is regarded as the earliest and most common manifestation of autonomic dysfunction in Parkinson's disease [10]. Change in the frequency of bowel movements in Parkinson's disease may be attributed to reduced salivary secretion, lack of physical exercise, reduced tones of both diaphragm and abdominal musculature, insufficient intake of fluid and anticholinergic medication, though it is somewhat controversial [10]. In addition, she underwent total hip replacement one month earlier, which inevitably resulted in a bed-ridden status with progressive constipation. The pathophysiology of stercoral perforation is considered to be formation of fecaloma causing pressure necrosis of the colon wall, leading to ulceration, and, ultimately perforation, usually located in the anti-mesenteric border of the descending colon, where the bowel wall has the lowest blood supply and the narrowest diameter [3].
The diagnosis has been reported to pose a challenge to surgeons because approximately one fifth of stercoral perforations of the colon may present with local peritonitis or vague abdominal pain [5]. The most useful tool for diagnosis of stercoral perforation is abdominopelvic CT [9]. Discontinuity in enhancement of the bowel wall in relation to focal fecal distension of the colonic lumen could represent a stercoral perforation [2]. However, in the present case, correct diagnosis of a stercoral perforation was difficult, because precise preoperative evaluation of integrity of colonic wall enhancement was not possible. Therefore, when evaluating patients with diffuse abdominal pain along with a history of long-standing bed rest and progressive constipation, stercoral perforation should be taken into consideration as one of the possibilities.
For treatment of a stercoral perforation, resection of the involved colon and proximal colostomy was known as the treatment of choice [3]. In addition, segmental resection of the diseased colon with anastomosis and diverting enterostomy or primary repair of perforated site with sigmoid loop colostomy could be successfully performed in some selective patients with limited intra-abdominal sepsis [1,3]. Evacuation of impacted fecaloma and identification of additional stercoral ulcers may result in avoidance of re-perforation and further complications. In our case, in the first operation, the perforation site was small and relatively well margined. The patient was severely undernourished, in that body mass index of the patient was only 13.3 kg/m2, therefore, we wanted to reduce the duration of anesthesia. We evacuated fecaloma near the perforation site, and performed primary repair of the perforation site with protective ileostomy formation. However, the primary repair site was not intact, which resulted in a second exploration and evacuation of impacted fecaloma in a more distal area using colotomy on the sixth postoperative day of the first surgery.
This report emphasizes that, for patients with peritonitis combined with a history of severe constipation, stercoral perforation should be taken into consideration. In addition, surgical treatment should include thorough evacuation of fecaloma with resection of the colon, including the perforation site, as well as copious intraperitoneal lavage for prevention of abdominal sepsis.
 XML Download
XML Download