

 Citation
Citation Print
Print


INTRODUCTION
The choledochal cyst can be defined as a congenital anomaly of the biliary system, characterized by cystic dilatation of the intrahepatic duct and the extrahepatic biliary tree individually, or cystic dilatation of both these parts simultaneously [1]. It has been reported that the incidence of choledochal cyst in Western countries ranges from 1:100,000 to 1:150,000 live births, and its incidence in Japan has been frequently reported to be 1:1,000 live births [2]. However, the precise incidence of choledochal cyst in Korea has not been reported so far. It has been known that choledochal cysts are caused by two main factors, namely, weakening of the bile duct walls and an obstruction distal to it. In addition to the causes of this disease, a close relationship between the choledochal cyst and pancreaticobiliary malunion (PBMU) has also been revealed [3]. Also, the probability of occurrence of PBMU related to the position of the opening of the papilla of Vater and the probability of the occurrence of choledochal cyst related to such a situation has been considered to be one of the causes, and recently a series of reports have been made available [3,4]. In this connection, we report our experience of choledochal cyst with PBMU and the papilla of Vater positioned in the third portion of the duodenum, in a 30-month-old boy.
CASE REPORT
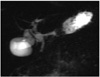
A 30-month-old boy, who was suffering from vomiting and abdominal pain since the past 20 days, underwent abdominal computed tomography (CT) scans at another hospital and was then transferred to our hospital under the impression of choledochal cyst. There was no particular past medical history or family history, except for the history of hospitalization for treatment of pneumonia one month prior to being admitted to our hospital. Physical examination revealed mild tenderness with rigidity in the right upper abdomen. Laboratory data including complete blood count and urinalysis were within the normal limits, but blood biochemistry revealed the following: aspartate aminotransferase 121 IU/L, alanine aminotransferase 155 IU/L, alkaline phosphatase 499 IU/L, gamma-glutamyl transpeptidase 168 IU/L, amylase 292 IU/L and lipase 129 U/L, showing elevated levels and T-bilirubin/D-bilirubin were 0.59 mg/dL and 0.16 mg/dL respectively, showing normal levels. Abdominal CT demonstrated dilatation of the extrahepatic bile duct and central dilatation of the intrahepatic bile duct (Fig. 1). Also magnetic resonance cholangiopancreatography demonstrated findings similar to abdominal CT but it could not identify the PBMU (Fig. 2). On biliary scan, the hepatic uptake appeared to be within the normal range, however, the accumulation of isotope at the common bile duct (CBD) and delayed excretion into the duodenum were confirmed based on the findings.
Under the diagnosis of choledochal cyst the operation was carried out, and the P-B type of PBMU, in which the pancreatic duct joins the CBD, and the papilla of Vater is positioned in the third portion of the duodenum were identified through the operative cholangiography (Fig. 3). Based on the operative findings, the diagnosis of a type I choledochal cyst was confirmed, and hence excision of the choledochal cyst and, Roux-en-Y hepaticojejunostomy were carried out. The patient was discharged on postoperative day 11 without any problems and in good general health condition.
DISCUSSION
Choledochal cysts are congenital anomalies of the biliary system and consist of cystic dilatation of the extrahepatic biliary tree, intrahapatic biliary ducts or both [2]. Based on the clinical and anatomic findings of choledochal cysts, Todani and others argued that choledochal cysts can be divided into 5 major types and these types can be further divided into 3 subcategories. Despite their classification into many types, the surgical method of treatment for each type is not far different from the conventional method of treatment for choledochal cysts [2]. Many studies on the pathogenesis of various types of choledochal cysts and their relationship with the adjacent structures are in full swing and are being reported. And in cholangiographic techniques, there has been a series of reports which suggest that there is a high possibility of a relationship between the choledochal cyst and PBMU [3]. A hepatic diverticulum appears in the ventral wall of the primitive midgut early in the 4th week of intrauterine life in the development of the human embryo. The extrahepatic bile duct system and the ventral pancreas arise from the hepatic diverticulum during the 4th to 6th week of intrauterine life. The dorsal pancreatic bud appears opposite the hepatic diverticulum [4,5]. The main duct of the ventral pancreatic bud develops near the entry of the CBD into the duodenum. As the duodenum rotates to the right and become C-shaped, the ventral pancreatic bud is carried dorsally with the bile duct. The superior ventral branch of the ventral pancreas joins the distal portion of the dorsal pancreatic duct to form the main pancreatic duct, which merges with the CBD, inserting into the duodenum via the papilla of Vater [4]. The papilla of Vater is generally situated halfway down the medial wall towards the posterior aspect of the descending or second part of the duodenum [3]. There have been rare cases in which the papilla of Vater was found in a position other than its normal position and such cases have been reported sporadically. However, such cases are interesting in the anatomical context [6,7]. Especially, very few cases have been reported in which the papilla of Vater opens in the third portion of the duodenum [8-10]. In a series of recent studies, it has been reported that the frequency of choledochal cyst in patients was higher when the papilla of Vater was positioned distal to its normal position [3]. In this context from the anatomical viewpoint, the ectopic distal location of the papilla of Vater represents the ectopic distal budding of the hepatic diverticulum during early embryonic life, it is straightforward to postulate that the longer distance between the ventral and dorsal pancreatic buds may result in a delay in communication of the ventral duct with the dorsal duct or failure of communication [4]. And also the formation of PBMU at the early embryonic stage is caused by canalization of ventral pancreatic duct and the anomalous union of pancreaticobiliary duct, which originate from the dislocation of the ventral pancreas, and it is also caused by the stretching of primitive common channel and CBD in accordance with the lengthening, which will result in a long CBD and a long common channel. Therefore, if growth of the epithelium in the CBD, the common channel and the pancreatic duct fails keep up with this anomalous elongation during fusion, the ducts may become attenuated, resulting in stenosis and weakness of the duct walls, and subsequent dilatation of the ducts, a phenomenon that has been observed clinically [4]. This suggests that the lengths of the common channel and the CBD in patients with choledochal cyst correlate strongly with the location of the papilla of Vater, i.e., the more distal the papilla of Vater is, the longer the common channel and the CBD [3].
In conclusion, we have reported a case of a 30-month-old child with choledochal cyst, in whom the form of PBMU occurred simultaneously and the papilla of Vater was positioned in the third portion of the duodenum. There is no difference in the conventional surgical method of treatment in such cases despite the variation in the opening position of the papilla of Vater. But the likely relationship between the opening position of the papilla of Vater and choledochal cyst should be considered when a variation in the opening position of the papilla of Vater is detected before surgery.


 XML Download
XML Download