

 Citation
Citation Print
Print


INTRODUCTION
Appendicular torsion, which was first described by Payne in 1918, is an infrequent cause of acute abdomen syndrome. Despite its rarity, sufficient cases have been reported in the literature to affirm that its presentation is practically identical to acute appendicitis [1]. Torsion of the appendix could be a primary event or an event secondary to other pathologies. In cases of primary torsion, a specimen examination shows secondary ischemic or necrotic change and luminal dilatation distal to the torsion site without any primary lesion. Gopal et al. [2] postulated that the contributing factors are a long appendix and a fan-shaped mesoappendix with a narrow base, which is usually attached to the appendix laterally. On the other hand, secondary torsion is caused by an appendiceal abnormality, such as, fecalith [3], cystadenoma [4], mucocele [5], a carcinoid tumor [5], adhesion [6], or lipoma [7]. Here, we report a case of secondary torsion of the vermiform appendix with mucocele, and review the literature on secondary appendiceal torsion.
CASE REPORT
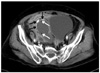
A 78-year-old female patient presented to the emergency room complaining of intermittent abdominal pain for 6 days, accompanied by nausea and vomiting for 2 hours. Her medical history included well-controlled diabetes mellitus for 15 years and no previous abdominal operation. The pain was located over the right lower quadrant of the abdomen. She had no change in bowel habits, bloody stools, or tenesmus. On physical examination, she was febrile, and had a pulse rate of 98 beats/min and a blood pressure 140/80 mmHg. A mass was palpated over the right lower quadrant with direct and rebound tenderness. The psoas sign was positive. Decreased bowel sounds were noted during auscultation. Laboratory findings were almost normal, except for the white blood cell count and hemoglobin (red blood cell count 303 × 104/mm3, hemoglobin 9.9 g/dL, hematocrit 28.6%, platelets 37.5 × 104/mm3, and white blood cell count 13,200/mm3). Serum analysis returned the following; total protein 7.4 g/dL, aspartate aminotransferase 22 U/L, alanine aminotransferase 10 U/L, blood urea nitrogen 24.0 mg/dL, and creatinine 1.4 mg/dL. Enhanced abdominal computed tomography depicted a hypoattenuated, well-encapsulated, 8 × 2 cm sized mass with smooth regular walls in the right lower quadrant with multiple calcifications and intra-luminal gas (Fig. 1). The radiologist suggested appendiceal mucocele with periappendicitis. The patient underwent surgery under a diagnosis of appendiceal mucocele with periappendicitis. During exploratory laparotomy, the greater omentum was found to be adherent in the right iliac fossa, and the appendix was found to be grossly distended and inflamed. The appendix was located in the pelvis and the base of the mesoappendix was narrow. The cecum was mobile, and torsion of about 900 degrees in the anticlockwise direction was noted just distal to the base (Fig. 2). Appendectomy and drainage were performed uneventfully. Grossly, the appendix was approximately 10.5 cm long and 4.7 cm in diameter distal to the site of torsion (Fig. 3). Histopathology showed that the lumen of the appendix was dilated and contained large amounts of mucus-like material, but there was no evidence of malignancy (Fig. 4). The postoperative course was uncomplicated, and the patient was discharged fourteen days later in good general condition.
DISCUSSION
Torsion of the vermiform appendix is a rare condition that clinically simulates acute appendicitis. The condition is indistinguishable preoperatively from acute appendicitis and it is invariably diagnosed intraoperatively [8]. The site of torsion is variable and could be at the base or about 1 cm or more distal to the base [8]. Furthermore, the position of the appendix is variable, but is usually described as free-lying or pelvic (as in our case) [2]. Primary and secondary torsion of the vermiform appendix have been described.
Primary torsion appears to be associated with anatomical variations, such as, a narrow base, a long appendix, or a fan-shaped mesoappendix [9]. Primary torsion of the vermiform appendix remains a rare finding that is usually found at surgery under another diagnosis-most commonly acute appendicitis. The origin of primary torsion remains unknown. Among cases with acute inflammation, the inflammatory response has been deemed an event secondary to torsion, rather than a precipitating cause [10]. On the other hand, secondary torsion has been reported to be associated with appendiceal abnormalities, such as, fecalith, cystadenoma, mucocele, carcinoid tumor, adhesion, or lipoma. Secondary torsion is much rarer and only 17 cases have been reported (from 1918) in the English literature. In the described case, the appendix was distended with purulent secretions and mucocele, which was considered a secondary factor of torsion. The mean age of patients with secondary torsion described in the literature is 43.8 years with a range of 16 to 79 years. No evident gender effect is evident, to date 9 female and 7 male cases have been reported. All patients presented with a complaint of right lower quadrant pain and most of nausea or vomiting. The direction of the appendiceal torsion was counterclockwise in about half of reported cases and reported degrees of appendiceal torsion vary from 180 to 1,080° with a mean 577°. Specimen measurements reveal an abnormally long appendix of mean length 10.7 cm. All reported cases were treated by appendectomy and achieved excellent outcomes.
In conclusion, torsion of the vermiform appendix is a rare disorder with an unclear etiology, and causes abdominal symptoms clinically indistinguishable from acute appendicitis. Its presentation is so variable that preoperative diagnosis is extremely difficult, and it is treated by appendectomy. Although appendicitis is the most common intra-abdominal surgical emergency, torsion of the vermiform appendix has only rarely been described, and is an uncommon cause of an acute abdomen. When a patient presents with abdominal pain indicating appendicitis, torsion of the vermiform appendix should be considered in the differential diagnosis.



 XML Download
XML Download