

 ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The causes of rectal stricture are diverse. Excluding causes by disease progression, iatrogenic causes occur due to chemical agents such as caustic materials and thermal injury. Intrarectal injection of harmful materials is responsive within several hours and the range of the injuries varies [1]. However because of its rarity, rectal burn has been poorly studied. Some have reported that hot water enemas for relief of constipation was the cause for rectal burns [2,3]. In most cases, after patients undergo a hot water enema to treat their constipation, they suffer from rectal stricture caused by rectal burn. The patients recovered without permanent rectal stricture by conservative treatment including a liquid diet plus dexamethasone suppository. However, despite the various conservative treatments, the patient in our case suffered from a persistent rectal stricture. We will report our experience of treating the intractable rectal stricture by rectal burn irresponsive to conservative treatments through surgery.
CASE REPORT
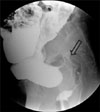
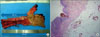
A 52-year-old woman who had used various methods to treat her chronic constipation underwent hot water enema about one month ago. However anal pain and constipation became aggravated prompting her to visit our clinic. On her physical examination, second-degree burn scars were found on both of her buttocks (Fig. 1). A flexible sigmoidoscopy revealed a severe nodular appearance with cicatrical changes around whole rectal wall and could not be advanced above 12 cm from the anal verge due to a severe concentric luminal narrowing (Fig. 2). An imaging study using contrast enema showed diffuse luminal narrowing with mucosal nodularity in the rectum and distal sigmoid colon and distension of the proximal bowel from diseased segment (Fig. 3). The result of mucosal biopsy came back as ulceration with granulation tissue. To relieve her colonic obstructive symptoms, a balloon dilatation was tried but failed, then a rectal stent was inserted with plans to retain for 2 months. However, at two months after rectal stent insertion, edema and erythema of the rectal mucosa still existed on colonoscopy (Fig. 4). At three weeksafter the removal of the stent, inflammation with severe edema and erythema of the rectal mucosa, ulceration, and easy-touch bleeding did not improve and the luminal narrowing had been aggravated (Fig. 5). Therefore we performed the surgical intervention of laparoscopic abdominal andtransanal proctosigmoidectomy with coloanal anastomosis with ileal diversion to treat her intractable rectal stricture and anal pain. Fig. 6 shows the operative specimen and histologic finding. The patient was discharged on her 10th postoperative day without any complication. The ileal diversion was buried three months later. After obtaining institutional review board approval (Subject No. VC10RISI0124), this case was reviewed.
DISCUSSION
Various barriers have to be overcome before colonic mucosa is thermally damaged: anal sensation, specifically anal skin sensation, is me diated by somatic efferent nerves and is sensitive to heat. Thermal injury to the upper gastrointestinal tract is rare, because any hot substance reaching the mouth is immediately expelled. However, the rectum is sensitive only to stretch and pull and not to direct thermal stimuli [4]. Therefore the rectum is very vulnerable to thermal injuries such as hot objects introduced into the rectum through voluntary actions that could skip anal protective mechanisms including anal contraction.
Patients suffering from chronic constipation have occasionally used various enemas. Of them, warm tap water or warm saline enemas are commonly preferred [5]. Hot water enema may be used with the misunderstanding that a hot substance would act as a stronger stimuli helpful for evacuation of stool or by the care of holistic practitioner [3]. In this situation because of direct thermal stimuli to the rectum, the probability of the rectal burn is high.
Most mucosal injuries in the rectum caused by thermal stimuli were well treated b y conservative methods including bowel resting and antibiotics, stool softeners, liquid diet and steroid suppository [2,3,6]. Although few reports were available, severe complication (i.e., bowel perforation, persistent bleeding, or bowel obstruction due to persistent rectal stricture) caused by thermal injury could not be found. Most cases were second-degree burn on the rectal wall, reporting that patients improved after two or three weeks of conservative treatment. Also, they indentified any improved rectal wall by sequential colonoscopy.
A rectal stricture may be defined as a chronic narrowing or obstruction to the flow of intestinal contents resulting in clinical symptoms or signs of complete or partial bowel obstruction [7]. A rectal burn with mucosal injury that is irresponsive to conservative treatment may be included as rectal stricture according to above definition. Therapeutic options for rectal stricture include dilatation, stenting, surgery, and so on. Many different treatments suggest that no one specific method is adequate for all strictures. Of them, the commonest reported method of mechanical dilatation of strictures is balloon dilation. For short rectal strictures, balloon dilation is a quick, simple, and adequate treatment for many patients. Although balloon dilation is relatively simple, it occasionally needs repeat procedures [8]. It is not clear how frequently dilations should be performed. Endoscopic stents have been used as a primary therapy with no other treatment or as a temporary measure to stabilize obstructed patients before semielective resection surgery. However, the application of stenting to benign rectal narrowing is uncommon. Stenting as means of treating benign stricture requires further evaluation. Operative treatment for rectal stricture is indicated to patients who have undergone multiple failed dilations and persistent rectal stricture after endoscopic stent. Also, patients with the rectal stricture involving a long segment of bowel would benefit from operative treatment. Operative treatment may be classified into two options: transanal approach and transabdominal approach. Operative methods through transanal approach are transanal strictureplasty with transanal endoscpic microsurgery or via flexible sigmoidoscopy, laser ablation, and transanal electrocautery. However, only a minor number of strictures are suitable for treatment via these methods. Higher and longer strictures would be technically difficult to treat in these ways. Garcea et al. [9] suggested that longer rectal strictures with multiple recurrences would require an open resection.
In our case, initially, her rectum was severely inflamed and already stenosed. The range of inflammation and stricture was a very long segment starting from distal sigmoid colon to entire rectum. The obstructive symptom improved right after the endoscopic stenting, however two months after the stenting, the obstructive symptom redeveloped. Her symptom after the removal of the stent was less improved instead aggravated; the elective operation for the intractable rectal stricture was planned. Because of the long-segment stricture, we planned surgical resection of involved segment and anastomosis with diversion. Using laparoscopic approach, abdominal and transanal proctosigmoidectomy with coloanal anastomosis with ileal diversion was performed successfully.
In conclusion, a rectal burn caused by hot water enema that is irresponsive to conservative treatment and progresses to chronic rectal stricture, corrective surgery such as resection of involved segment with anastomosis may be beneficial in relieving obstructive symptoms.




 XML Download
XML Download