

 ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Inguinal hernioplasty is one of the most frequent general surgery operations. Many operative versions have been reported. Tension-free inguinal hernioplasty was first reported in 1989 [1]. The approach has since become the standard procedure worldwide. As a minimally invasive laparoscopic surgery technique, laparoscopic hernia repair was introduced in the early 1990s [2,3], and has also become popular worldwide. The debate concerning conventional tension-free inguinal hernioplasty and laparoscopic inguinal hernia repair has been spirited. Several studies reported a trend towards an increase in hernia recurrence following laparoscopic hernia repair compared with conventional hernia repair, but this difference was not significant [4,5]. Yet, in the hands of surgeons experienced with laparoscopic hernia repair, the recurrence rate is similar for both procedures [6]. Laparoscopic hernia repair has been reported to be superior to conventional inguinal hernioplasty with respect to reduced postoperative pain, earlier return to work, and a better cosmetic outcome [4,5].
In recent years, various kinds of single port laparoscopic surgery have been reported including appendectomy and cholecystectomy [7,8]. Various ingenious single port laparoscopic surgical variations are being attempted in various surgeries including hernia repair. However, few reports of single port laparoscopic total extraperitoneal (TEP) hernioplasty have been published.
The present study chronicles the introduction and experience with single port laparoscopic TEP hernia repair.
METHODS
During the 10 months following June 2010, 63 cases of single port laparoscopic TEP hernia repair of inguinal hernias in 60 patients were performed at Incheon St. Mary's Hospital, The Catholic University of Korea School of Medicine. The operation was performed by one surgeon whose experience includes over 100 cases of conventional three port laparoscopic TEP hernia repair and more than 70 cases of single port laparoscopic appendectomy. Patient demographics, clinical data, intraoperative findings, and postoperative course were prospectively collected. This study was approved by the hospital's Institutional Review Board. All patients underwent surgery after providing informed consent.
Surgical technique
Under endotracheal general anesthesia, each patient was placed in the supine position with both arms adducted. A monitor was placed on the side of the hernia, with the surgeon and camera operator standing on the opposite side. Each patient was placed in a Trendelenburg position and the opposite side of the hernia site was tilted down. In 30 early cases, we used oblique incision to hernia site. But, in 30 late cases, we used vertical incision because of cosmetic effect and approach to bilateral hernia. A single 2 to 2.5 cm-long incision was made on the midline, beginning from the deepest part of the umbilicus and extending to 0.5 to 1.5 cm of the periumbilicus. The subcutaneous layer was dissected down to the anterior rectus sheath and the anterior rectus sheath was incised transversely, approximately 2.5 cm long. After the splitting of the rectus muscle, our previously described glove single-port device [7,8] was inserted in front of the posterior rectus sheath (Figs. 1, 2). Carbon dioxide was insufflated to 12 mmHg. The preperitoneal dissection was performed using a rigid, 30-degree, 5 mm laparoscope and two Blunt dissectors (Ethicon Endo-Surgery Inc., Cincinnati, OH, USA). Almost all the procedures were performed using the same method with conventional laparoscopic TEP repair using a standard laparoscopic instrument.
Direct hernia was completely reduced with gentle traction. Transversalis fascia ('pseudo-sac') was anchored on the pubic bone by titanium tacks (Tacker, Covidien plc, Dublin, Ireland) to prevent seroma formation. Dissection of all possible hernia sites was performed to eliminate the possibility of missed hernias.
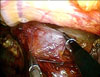
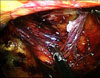
In the case of an indirect hernia, the sac was separated from the cord structure by the spread technique. In case of right indirect hernia, an Endo Grasp (Covidien plc) held in the left hand was used to grasp the sac and push it to the lateral side, and the right hand was used to dissect the cord structures by pushing the medial side, keeping dissection close to the sac (Fig. 3). The sac was isolated by a repeat of this motion. In the case of a left hernia, the procedure was mirror imaged to the right side. In a large scrotal type of hernia, the sac was incised beyond the internal ring and closed with vicryl Endo-loop (Sejong Medical Co., Paju, Korea). After completion of sac dissection and isolation (Fig. 4), the cord structures were freed from the peritoneum (parietalisation).
Afterwards, a surgical glove was detached and a 13 × 9 cm Parietex (Covidien plc) mesh was inserted through a single incision. After the mesh was positioned properly, two tacks were placed in the Cooper's ligament and the anterolateral abdominal wall. The space was deflated, with care taken not to displace the mesh. The anterior rectus sheath was closed using continuous 2-0 Vicryl sutures. The single skin incision was closed with subcuticular sutures.
RESULTS
Single port laparoscopic TEP hernia repair was successfully completed in 60 patients. Patient demographics and hernia characteristics are summarized in Table 1. The overall mean age of the patients was 58.5 years (range, 24 to 85 years) and mean body mass index was 23.3 kg/m2 (range, 17.6 to 27.6 kg/m2).
Operative and post-operative data are summarized in Table 2. Mean operative time was 62.0 minutes (range, 32 to 150 minutes). Mean operative time of indirect hernia was 65.2 minutes and direct hernia was 52.6 minutes. Mean operative time of both inguinal hernia was 77 minutes. None of the patients experienced intraoperative complications. There was one conversion to conventional transabdominal pre-peritoneal (TAPP) hernioplasty due to omental incarceration, which was severely adhered to the sac. Two postoperative complications occurred: one wound seroma and one urinary retension. Both were treated conservatively. Mean post-operative hospital stay was 2.15 days.
DISCUSSION
The two most common techniques in laparoscopic hernia repair are TAPP and TEP hernia repair. The TAPP approach is considered to be easier to perform than TEP repair. There is no difference in terms of recurrence, time to normal activity and time to work between the two procedures. However, the TAPP approach carries the potential risks of visceral injury, intestinal obstruction and port-site hernia [4,9-12]. One study reported that the risk of intestinal obstruction following TAPP procedure was 1.14 per 1,000 personyears and 0.28 after TEP procedure [13]. In case of single port laparoscopic TAPP hernia repair, completely scarless-transumbilical single incision is possible [14]. However, in case of TEP, completely transumbilical incision is technically challenging due to the difficulty in approaching the anterior portion of posterior rectus sheath. For that reason, although we used the umbilicus as a single port access, a portion of the incision (0.5 to 1.5 cm) was extended outside of the umbilicus. However, the umbilical portion of the incision was invisible and the operative scar was nearly invisible (Fig. 5). In our opinion, our unique umbilical incision is cosmetically superior to the previously reported 2.5 to 3 cm-long infraumbilicus incision [15-17]. In this study, there was 3.3% minor morbidity: one case of wound seroma and one case of urinary retension. In the case of wound seroma, we divided the sac due to large scrotal hernia. The seroma was completely resolved on an out-patient basis after five rounds of aspiration. In the case of the urinary retension, the patient had suffered from benign prostate hyperplasia. After 3 days of urinary drainage, voiding was acceptable. Another study reported a 2.1% incidence of hematoma or seroma, and incidence of urinary retension of 0.2% [18]. Still, more cases are needed to accurately establish the morbidity rate in single port TEP hernioplasty.
Many surgeons perform single port surgery using an articulating instrument. However, we did not use an articulating instrument due to the restricted operating space of the TEP procedure, and operational difficulty of the articulating instrument.
Presently, single port TEP repair is performed with the same method and instrument as used for conventional TEP repair. Despite this similarity, intraoperative complications, morbidity, recovery, pain and recurrence could differ. Large scale, controlled randomized trials are needed to establish the short-term and long-term outcomes between single port and conventional laparoscopic TEP repair.
We report the safe use of single port laparoscopic TEP hernioplasty. With the improvement of the single port laparoscopic instrument, single port TEP hernia repair should become more comfortable and less time-consuming to perform.
In conclusion, single port TEP repair is feasible and safe. Umbilical incision provides excellent cosmetic outcomes. A prospective randomized study comparing single port TEP with conventional TEP is necessary to establish the safety and long-term results of single port TEP hernioplasty.




 XML Download
XML Download