

 ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Although the incidence of gastric carcinoma is declining in the general population [1,2], its incidence in the elderly is increasing [3,4]. In conjunction with recent increases in life expectancy, more of these patients are undergoing surgery for gastric carcinoma than in the past. Despite advances in operative techniques [5,6], the prognosis of patients with gastric carcinoma invading the serosa remains poor [7,8].
Since the incidence of gastric carcinoma in the elderly is also increasing, we are interested in the clinicopathologic features and prognostic factors that affect the survival rate of elderly gastric carcinoma patients with serosal invasion. This study analyzed the clinicopathologic features of gastric carcinoma patients with serosal invasion older than 70 years and compared them with young patients.
METHODS
Patients and specimens
From 1991 to 2004, 2,032 patients with gastric carcinoma were admitted to the Division of Gastroenterologic Surgery. Of these, 136 were in the elderly group (defined as older than 70 years of age). All patients had a primary adenocarcinoma of the stomach and had no evidence of any other malignancy. The clinicopathologic features of these elderly gastric carcinoma patients with serosal invasion were reviewed retrospectively. Information on each patient's age, sex, extent of lymph node dissection, operative curability, type of surgery, tumor size, tumor location, Borrmann type, histologic type, nodal involvement, hepatic metastasis, peritoneal dissemination, stage at the initial diagnosis, and survival rate was obtained from the hospital records. A histological evaluation was performed according to the Japanese General Rules for Gastric Cancer Study in Surgery and Pathology [9]. Curative resection was defined as all gross disease removed as judged by the surgeon at operation.
Statistical analysis
Statistical analysis was performed using the SPSS ver. 12.0 (SPSS Inc., Chicago, IL, USA). The survival rates of the patients were calculated using the Kaplan-Meier method and the relative prognostic importance of the parameters was investigated using the Cox proportional hazards model. The chi-square test was used to evaluate the statistical significance of differences, and P-values less than 0.05 were considered significant.
RESULTS
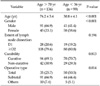
Of the 2,032 patients, 136 aged > 70 years were classified as elderly patients. There were 91 males and 45 females; the gender ratio was 2.02:1. The age of the patients at the time of the initial diagnosis ranged from 71 to 84 years old, with a mean age of 74.2 years old. Subtotal gastrectomy was the procedure most frequently performed (66.9% of cases) in elderly patients, but total gastrectomy was frequently performed in the younger group (50.5% vs. 25.7%; P < 0.05) (Table 1).
Table 2 summarizes the histopathological features of elderly gastric carcinoma patients with serosal invasion. The lower third of the stomach was the most common site of gastric carcinoma in both groups, and the upper third was more frequently involved in the young than in the elderly (28.3% vs. 10.3%; P<0.01). Significantly more old patients had a well- or moderately differentiated histology and more young patients had a poorly differentiated histology and signet ring cell carcinoma (P < 0.001). Borrmann type IV lesions were more common in younger patients than in the elderly group (22.2% vs. 11.8%; P < 0.05). Multivariate analysis showed that two factors were independent, statistically significant parameters associated with survival: histologic type (risk ratio, 1.805; 95% confidence interval [CI], 1.041 to 3.132; P < 0.05) and operative curability (risk ratio, 2.506; 95% CI, 1.371 to 4.581; P < 0.01) (Table 3).
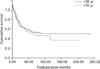
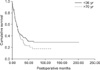
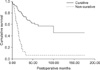
The 5-year survival rates of the young and elderly patients with serosal invasion did not differ statistically (37.5% vs. 27.8%; P = 0.295) (Fig. 1). The 5-year survival rates of young and elderly patients with curative resection did not differ statistically (43.3% vs. 33.9%; P = 0.318) (Fig. 2). The elderly patients with curatively resected gastric carcinoma had a better survival rate than the elderly patients with non-curatively resected gastric carcinoma (52.1% vs. 7.8%; P < 0.001) (Fig. 3).
DISCUSSION
Gastric carcinoma is usually a disease of the aged, and patients have a mean age over 60 years [10,11] and the incidence of gastric carcinoma is increasing in very old patients (>70 years) [2-4]. There is controversy as to whether gastric carcinoma in elderly patients differs from that in young patients. Some authors have reported an inverse relationship between age and prognosis in gastric carcinoma [3,5]. We reviewed patients with serosa-positive gastric carcinoma retrospectively to compare the clinicopathologic features in elderly and young patients.
In the present study, there was a significant difference in the sex ratio between the elderly and young patients. In the elderly patients, there was a higher proportion of male patients (2.02:1 in this study). Several studies have obtained the same results [1,12]. The causes of this sexual imbalance are not yet clear. We proposed that possibly, sex hormones may play a role to gender predilection. Some authors suggested that male patients may have more frequent and prolonged exposure to environmental carcinogens than females, which might explain the male predominance among elderly patients [13]. By contrast, there was a higher proportion of female patients in young patients.
Concerning the tumor location, the incidence in the lower third of the stomach was higher in elderly patients than in young patients. It was reported that the same results [14]. Some investigators found that the location of tumor had a significant impact on survival [12]. In contrast to their result, we found that tumor location was not a significant prognostic factor in elderly gastric carcinoma patient with serosal invasion by multivariate analysis.
By histologic type, we found that significantly more elderly patients had a well or moderately differentiated histology, and more young patients had a poorly differentiated histology (P < 0.001). Other studies have reported similar results [1,3,4,12,14], and this may due to lack of carcinoma cell differentiation in the young patients. It was reported that the histologic type of early gastric carcinoma in elderly patients; 45.5% of early gastric carcinoma was well-differentiated adenocarcinoma [15]. In contrast to elderly patients, the higher incidence of poorly differentiated adenocarcinoma in young patients found in this study is consistent with the literature. In this study, histologic type was one of significant prognostic indicator in multivariate analysis.
Some investigators found that the presence of lymph node metastasis plays an important role in predicting the prognosis in patients with gastric carcinoma [16,17]. In the current study, there were no significant differences in either lymph node invasion between the two groups and lymph node metastasis had no affect on prognosis of elderly gastric carcinoma patients with serosal invasion. Some authors demonstrated that serosal invasion is another important prognostic factor in addition to lymph node metastasis [16,18]. However, our previous results found that serosal invasion did not emerge as an independent, statistically significant prognostic parameter for node-positive gastric carcinoma patients with curative resection who showed long-term survival [4].
Surgery is the only potentially curative modality for localized gastric carcinoma. In accordance with most literature reports [11,14,19], curative resection offered the only chance of long-term survival. It was reported that when the tumor was curatively resected, the prognosis was favorable in patients with gastric carcinoma patients [19]. Nevertheless, some authors concluded that the extent of surgery should be considered, especially as total gastrectomy and extended node dissection are associated with higher operative mortalities [20]. Many investigators have reported a low curative resection rate in elderly patients with gastric carcinoma [12,21,22]. In our series, however, the curative resection rate (69.1%) in the elderly group was much higher than previously reported in Western countries. It was reported that surgery should not be avoided based solely on the age of patient [23]. We also agree with their recommendation and perform gastrectomy with D2 lymph node dissection in elderly patients with advanced gastric carcinoma who have no medical illness, such as cardiovascular or respiratory problems to achieve curative resection. In contrary, some investigators recommended that the less extensive gastric surgery for the very old patients with gastric carcinoma to improve quality of life [24].
It was reported that there was a trend to more cases with stage IV in the group of young patients than in older patients (76% vs. 64%), although the difference was not statistically significant [12]. In contrast to their result, we found that stage IV gastric carcinoma was more in the group of elderly patients than in young patients (36.8% vs. 33.3%), and also the difference was not statistically significant in this study. This was due to delay in diagnosis in elderly gastric carcinoma patients.
Although the young patients presented aggressive histologic patterns, it was reported that there was no statistical difference in survival rates between the elderly and young gastric carcinoma patients [1]. In this study, the 5-year survival rates of the elderly and young patients did not differ statistically (46.5% vs. 52.8%). These findings suggest that elderly patients with gastric carcinoma can tolerate radical treatment well. The elderly patients with curatively resected gastric carcinoma had a better survival rate than the elderly patients with non-curatively resected gastric carcinoma (68.1% vs. 6.5%). By contrast, others [3,20,24] reported that the survival rates of the elderly were worse, both overall and after curative resection, than those of younger patients. Delay in diagnosis and a more advanced stage of gastric carcinoma in elderly patients have been suggested as possible causes. In a few reports, however, the prognosis of elderly patients who underwent curative resection was the same as that of young patients. Many investigators [4,22,25] also reported similar survival rates in the two age groups when the same tumor stages were compared.
In conclusion, elderly patients represent more differentiated histology compared to young patients. This study demonstrated that there was no significant differences in outcome of gastric carcinoma with serosal invasion between elderly and young patients. The prognosis of serosa-positve gastric carcinoma is not related to the patients' age.


 XML Download
XML Download