

 ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Lymphangioma is a benign form of lymphatic malformation usually resulting from blockage in regional lymph ducts. Pathologically, it exhibits protein and eosinophilic exudate inside the swollen cystic space in a thin layer surrounded by the endothelial cells. In most cases, lymphangioma develops during childhood, with varying symptoms according to the location of its development. The most frequent sites of the condition include the head and neck (75%) and the axilla (20%), with rare cases reported in the mediastinum, the mesothelium, the pericardium, the groin, and the intraperitoneum.
Intraperitoneal lymphangiomas occur most frequently in the in the mesenteric region and less frequently in the mesocolic, greater omental, and retroperitoneal regions, the small intestinal and gastric walls, and the peritoneum [1]. Occurrence of cystic lymphangioma in the pancreas is extremely rare, accounting for less than one percent of reported cases [2]. To date, about 60 cases have been reported world-wide [3].
To our knowledge, this is the rarely reported case of pancreatic cystic lymphangioma in Korea. Therefore, we report this successfully treated case of pancreatic cystic lymphangioma with a brief review of the relevant literature.
CASE REPORT
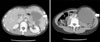
A 37-year-old woman was admitted to emergency services with complaints of left-sided abdominal pain which had persisted over two weeks, as well as a mass which had increased in size for several days. The patient was not receiving any specific medication and her medical history did not suggest any major disease. Nor was there any history of alcohol usage or trauma. Physical examination revealed the presence of a huge mass in the upper left quadrant of the abdomen, but without tenderness or rebound tenderness. Laboratory findings were all within normal limits. The abdominal X-ray examination showed no presence of intestinal gas in the upper left quadrant and the normal location of the intestines was pushed toward the right, indicating the presence of a mass in the upper left quadrant (Fig. 1). An abdomino-pelvic computed tomography (CT) scan demonstrated a 15 × 10 cm, hypo-dense, well-capsulated and huge cystic lesion of unknown origin in the upper left quadrant (Fig. 2).
A surgical procedure was decided upon because of compression symptoms and the possibility of the mass being malignant. Under general anesthesia, a median incision was performed in the upper abdominal region. The spleen appeared normal, while the presence of a mass was confirmed, firmly attached to the pancreatic tail. The mass was hard and uneven with tubercles of varying sizes. To perform en bloc resection of the mass, mobilization of the spleen was deemed necessary. Both the splenorenal and splenocolic ligaments were detached from the retroperitoneum to mobilize the spleen. After removal of the pancreatic tail and the spleen from the abdominal cavity, excision of the mass and the pancreatic tail, as well as splenectomy, were performed to ensure en bloc resection (Fig. 3). No other abnormalities were found inside the cavity after the procedure. The peritoneal cavity was irrigated thoroughly with normal saline solution and Jackson-Pratt drains were placed in the left subdiaphragmatic area and in the pelvis.
The removed mass had a clearly distinguishable outer membrane, a smooth, polished surface, and signs of swelling due to the liquid it contained (Fig. 4). The sectioned specimen contained mildly bloody serous liquids and a large swollen cyst. Small multiseptated cystic masses of various sizes were also seen situated along some of the thicker portions of the cystic wall. Pathologic findings showed that the mass was comprised of a number of multiseptated cystic masses of varying sizes that were wrapped with flat lymphatic endothelial cells. Some lymphatic infiltration was found in the mass. However, no connection with the pancreatic main duct was observed despite the firm attachment between the mass and the pancreas (Fig. 5).
At immunohistochemistry, the endothelial cells that made up the cyst showed a strong positive reaction to CD31 and D2-40 and a mild positive response to CD34. Based on the results of the microscopic and immunohistochemical findings, a diagnosis was made for a cystic lymphangioma consisting of lymphatic endothelial cells (Fig. 6).
The patient recovered uneventfully and was discharged on the 9th postoperative day. At the follow-up examination 3 months after surgery, she was doing well.
DISCUSSION
Cystic lymphangioma of the pancreas was first identified in 1913 by Koch [4] as a form of benign cyst secondary to blocked regional lymphatic ducts. It is extremely rare, accounting for less than 1% of lymphangiomas [3]. Frequently occurring in the pancreatic tail, the disease is reported more often in females, with a similar incidence across all age groups.
Several factors are assumed to cause cystic lymphangioma. These include lymphatic abnormalities resulting in children from sequestration of lymphatic tissues during prenatal development and in adults from blockage of lymphatic ducts due to abdominal trauma, operation, radiological treatment, or infection. Cystic lymphangioma can occur in any location where normal lymphatic ducts are found. The most frequently reported sites are the head and neck (75%), the axilla (20%), and other organs (5%). Cystic lymphangioma inside the abdominal cavity is very rare, occurring most frequently in the mesenteric region, and less frequently in the mesocolic, greater omental and retroperitoneal regions, small intestinal and gastric walls, and peritoneum [1]. Cystic lymphangioma of the pancreas is particularly rare, with only 60 cases reported so far world-wide [3].
Clinical symptoms of cystic lymphangioma found inside the abdominal cavity, if present, vary from no symptoms to a variety of symptoms depending on the location and size of the mass. More acute cases are reported in children whereas more chronic development is common among adults [1]. Features of pancreatic cystic lymphangioma normally involve abdominal pain and the presence of a mass confirmed by tactile examination. In this case, the patient was a female who complained of a chronic condition of abdominal mass with rapidly growing, of which the cause was later confirmed as pancreatic cystic lymphangioma.
Diseases requiring particular attention to accurate diagnosis include: pancreatic pseudocyst, mucinous cystadenoma, serous cystadenoma, cystic carcinoma of the Wirsung's Duct, and congenital neoplasms [5]. To ensure distinction between cystic lymphangioma and the aforementioned conditions, diagnostic tools such as plain abdominal films, abdominal CT, and magnetic resonance imaging (MRI) may be utilized. Plain abdominal X-rays may reveal dislocation or blockage of the intestines, and CT and MRI could help determine the pre-operational location of the mass, the relationship between the mass and its surrounding structures, the size of the mass, and likely complications of surgery. However, these tests do not guarantee a completely accurate diagnosis. It is still considered a difficult task to accurately diagnose pancreatic cystic lymphangioma prior to a surgical procedure [3,6,7].
Although normally considered benign, cystic lymphangiomas can continue to increase in size, infiltrate the neighboring organs, and pose risks for complications such as leakage of lymphatic fluids and recurrence. If the infiltrated organs are excisable, they must also be removed along with the mass itself with the aim of treatment being a benign excised surface on microscopic examination [6-8]. Our case, included the full excision of the mass, the pancreas (the origin of the mass), and the spleen connected to the mass. No complications, such as lymphatic liquid leakage, were seen after the procedure.
Diagnostic confirmation of pancreatic cystic lymphangioma is pathologically possible. On visual inspection, the mass would have clearly defined gray-reddish boundaries and a smooth outer membrane. Inside the mass, serous eosinophilic exudates would be observed. Microscopic examination would reveal flat endothelial cells bordering pancreatic tissues or ducts in the cystic membrane and diversified lymph cells in the cystic membrane or lymphatic ducts. Also, the pancreas is likely shrinked due to the pressure [4].
Immunohistochemistry can be used to increase the accuracy of diagnosis. Since the endothelial cells of the outer membrane of pancreatic cystic lymphangiomas do not normally undergo epithelial differentiation, staining materials, such as (periodic acid-Schiff) PAS stain, Mucicarmine, Alcian blue, and anti-cytokeratin are unsuitable. However, staining via immunochemical materials like Factor VIII-R Ag, CD31, CD34, and D2-40 is known to produce a response. Diagnosis of the disease, therefore, involves the use of such immunochemical materials [3,9]. In our case, pathological testing revealed a close proximity between the pancreas and multiseptated cystic masses of varying sizes that were comprised of lymphatic endothelial cells. The cells responded to staining using immunochemical substances like D2-40, CD31, and CD34, which allowed the diagnosis of pancreatic cystic lymphangioma (Fig. 6).
We therefore report this rare case in the hope that although extremely rare, cystic lymphangioma of the pancreas should be taken into consideration as a differential diagnosis of pancreatic cystic or retroperitoneal lesions, especially in women.





 XML Download
XML Download