

 ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The retrorectal space lies between the upper two-thirds of the rectum and the sacrum, above the rectosacral fascia, Waldeyer's fascia. It is also known as the presacral space. This space is an area of embryologic fusion and remodeling. And a heterogeneous group of both benign and malignant tumors originating from the embryologic remnants can be found in this space [1]. Retrorectal tumors in adults are very rare. However, most general surgeons can expect to encounter at least one adult patient with a retrorectal tumor during the course of their careers [2]. Most retrorectal tumors present without specific symptoms. Thus, these lesions are easily missed if the examiner does not maintain a high index of suspicion [2]. Although the majority are benign, they present a number of problems in preoperative diagnosis with imaging studies because there is debate and difficulty in concerning preoperative biopsy of these lesions [2,3]. Therefore, complete surgical resection is most important not only for treatment but also for exact diagnosis [4].
Recently, surgeons have become familiar with the pelvic anatomy by the accumulation of experiences of laparoscopic rectal surgery. Also, the laparoscopic approach has the benefit of avoidance of large abdominal skin incision.
The aim of this study is to review incidence, diagnostic tool, and treatment modality for retrorectal tumors in our hospital and to introduce the advantage of the laparoscopic approach for retrorecal tumor resection.
METHODS
In total, 15 patients who underwent surgical resection for retrorectal tumor in our hospital from May 2002 to April 2010 were reviewed retrospectively. Mean follow-up length was 16.1 months. After Institutional Review Board approval of our institute was obtained (Subject No., VC10RISI0126), patient's demographics including initial symptoms, preoperative diagnostic tools, treatment modalities, intraoperative and postoperative complications, characteristics of tumor, and data of postoperative course were reviewed. We defined the patient's condition as a recovery of usual activity when he or she ate a soft or regular diet, did not require analgesics for pain control, and could recover physical activity without difficulty in social life.
We performed three surgical approaches for resecting rectrorectal tumors. These included the abdominal or anterior approach, the transsacral or posterior approach, and the combined or abdominosacral approach. The operative approach was determined on digital rectal examination and radiologic findings. The anterior approach was typically performed for high lesions without evidence of sacral involvement. When the examiner's finger could not palpate the upper extent of the tumor, we performed resection of this high retrorectal tumor by anterior approach. With a lower midline skin incision, the sigmoid colon and rectum were mobilized, and then the retrorectal space was entered. We made a great effort to preserve the presacral nerves. Recently, we performed the laparoscopic approach in three patients, instead of open surgery. If the examiner's finger could palpate the upper extent of the tumor, we performed resection of this low retrorectal tumor by posterior approach. During the posterior approach, the entire or partial resection of the coccyx was always performed and the surgical wound was sutured after levatorplasty. If the examiner's finger could palpate the tumor well but the upper extent of the tumor could not be palpated, we performed resection of this large tumor by combined approach. After we performed the dissection and the mobilization of the upper extent of the tumor by anterior approach, the dissection of the lower part of tumor with resection of the coccyx and the removal of the tumor were performed posteriorly. In the latest case of combined approach, we removed the tumor posteriorly without an additional abdominal incision for tumor extraction after laparoscopic anterior approach.
Student's t-test and chi-square test were used for comparing patient characteristics between open transabdominal approach and laparoscopic abdominal approach. Statistical significance was accepted at P < 0.05. Continuous variables are expressed as the mean ± SD. The applied statistical software was SPSS ver. 12.0 (SPSS Inc., Chicago, IL, USA).
RESULTS
Table 1 shows the clinicopathological features of fifteen patients with retrorectal tumors. Two of fifteen patients were males and thirteen were females. The patients' ages ranged from 20 to 66 years, with a mean age of 45 ± 15.7 years. The most common symptom presented at first visit was a lower abdominal pain or discomfort (8 cases, 53.3%). Other symptoms were defecation difficulty (2 cases, 13.3%) and urination difficulty (2 cases, 13.3%). One patient was detected during operation for suspected ovary tumor proven to be a retrorectal tumor. Two patients (13.3%) were found during health screening tests for early detection of malignancy. Preoperative imaging modalities included computed tomography (CT) scan (10 cases, 66.7%), magnetic resonance imaging (MRI) (10 cases, 66.7%), transrectal untrasound (2 cases, 13.3%), and double contrast colon study using barium (1 case, 6.7%).
An anterior approach was performed in eight patients (53.3%) and a posterior approach with the excision of the coccyx in five patients (33.3%). A combined approach was performed in two patients (13.3%). A laparoscopic approach was performed in three of eight patients who underwent anterior approach and one of two patients who underwent combined approach. The largest diameter of the tumor in intraoperative findings ranged from 4 to 14 cm, with a mean largest diameter of 6.2 ± 2.9 cm. The perforation of cystic tumor during operation developed in three cases. No postoperative mortality was observed. Mean hospital stay after operation was 10.7 ± 6.1 days. Postoperative complications were chronic constipation in one, surgical site infection in one, and S1 radiculopathy in one.
The most prevalent postoperative histologic diagnoses were neurilemmoma (4 cases, 26.7%) and mature teratoma (4 cases, 26.7%). And the others were tailgut cyst (3 cases, 20%), epithelial cyst (2 cases, 13.3%), solitary fibrous tumor (1 case, 6.7%), and chondrosarcoma (1 case, 6.7%). There was no recurrence in fourteen benign tumors during the mean follow-up length of 13.6 ± 19.8 months. A pseudocyst formation was detected fourteen months after operation in one female patient with tailgut cyst. She was successfully treated by percutaneous drainage. The chondrosarcoma was the only malignant tumor in our study. The chondrosarcoma was resected by anterior approach. We performed the salvage surgery at postoperative month 23 due to local recurrence. In spite of additional chemotherapy after salvage surgery, she died at 51 months after first operation due to progression of the recurrent disease.
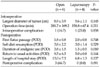
In the present study, transabdominal approach was performed in 10 patients including two patients who underwent combined approach. Four of these 10 patients underwent laparoscopic surgery. Comparing intraoperative and postoperative parameters between open transabdominal approach and laparoscopic abdominal approach, durations of required pain control with analgesics were shorter in patients who underwent laparoscopic surgery after surgery than open surgery (Table 2). And, laparoscopic surgery had a tendency to provide earlier postoperative recovery than open surgery.
DISCUSSION
Although their incidences were diverse according to published reports, there is a common point that retrorectal tumors are a very rare disease. Several reports that analyzed incidence of retrorectal tumor in some general hospitals spanned 19 to 55 years demonstrated that retrorectal tumors were detected in 0.9 to 6.3 patients per year [5-8]. The incidence at the Mayo Clinic, as reported by Jao et al. [7], has been found to be approximately one in 40,000 general hospital admissions. However, because most of these reports were conducted in major referral centers, the reported incidence may be much higher than in the general population. Hobson et al. [2] suggested that the average surgeon practicing outside the setting of a major referral center can expect to see at least one patient with a retrorectal tumor during the course of a typical career. Based on this suggestion, they emphasized that establishing the diagnosis requires an awareness of the possibility of a retrorectal tumor in any patient presenting with a posterior mass on rectal examination. In Korea, Kwon et al. [9] published their report with an incidence of 1.6 patients per year (10 patients for 6 years). In this study, we experienced 15 patients with retrorectal tumors over 9 years. About 1.7 patients were diagnosed with retrorectal tumor annually in our hospital. As this incidence is one per 1,500 surgeries performed under general anesthesia, this result is similar to the above mentioned reports.
Generally, the symptoms caused by retrorectal lesions are related to their site, size, and, in the case of retrorectal cysts, the presence or absence of infection [1]. The most common presentation of a retrorectal mass is an asymptomatic mass discovered on routine screening digital rectal examination. Although benign retrorectal tumors are more common among females than males, this finding might represent a selection bias because young females of childbearing age undergo digital rectal examinations far more frequently than their male counterparts [2]. Also tumors with infectious etiology might cause pain. Retrorectal tumors can frequently present with infection. This tumor can be diagnosed during the evaluation for intractable anorectal fistula or abscess. It is important that a high index of suspicion for the retrorectal tumor in this condition be necessary for the successful diagnosis and treatment [5]. In our study, lower abdominal pain or discomfort (53.3%) was the most common presenting symptom. The ratio of male to female was 2:13. We experienced one patient with a lesion similar to anal fistula at her first visit. After the lesion was diagnosed as a retrorectal tumor by preoperative work up for the anal fistula, she underwent surgery for the retrorectal tumor.
Although many imaging modalities were tried to diagnose retrorectal tumors and to establish the treatment plans, it has been widely known that CT scans and MRI are the most important modalities to date. CT scans are the most important means of evaluating sacral lesions and planning the operative approach [1,7,9]. In our series, CT or MRI were performed in most patients preoperatively and those were helpful for preoperative diagnosis and for planning the operative approach. We experienced two retrorectal tumors which were found incidentally. One was diagnosed by a screening test for early detection of gynecological malignancy, another for colorectal malignancy. We think that this result suggests that more screening tests for gynecological or colorectal malignancies lead to more chances of finding asymptomatic patients.
There is no place for preoperative biopsy of a lesion because a biopsy may cause seeding of malignant cells. And, if the lesion is a cyst, infection may ensue. The best biopsy is complete surgical excision [6,7]. Complete surgical excision is necessary not only to resolve patients' symptoms, but also to prevent the extension of infection or malignant transformation. Besides, complete surgical excision is necessary for exact histological diagnosis. Curative resection requires complete excision of the tumor, with an intact capsule for clinically benign well circumscribed lesions and en bloc resection with microscopically clear resection margins for malignant tumors [10]. The access and approach to the tumor depends on its location and size. Digital rectal examination is helpful for deciding the approach. An anterior approach is typically performed for high lesions without evidence of sacral involvement. During an anterior approach, the middle sacral vessels should be ligated before mobilization is attempted. An anterior approach has the advantage of providing excellent exposure of pelvic structures [1,11]. Most tumors with a proximal extent palpable on rectal examination are amenable to a posterior approach. If even half of the lesion can be palpated, the lesion can be approached posteriorly [1]. It has been recommended that the coccyx always be sacrificed, not only to achieve better exposure but because the most common factor in recurrence is failure to remove this bone [5]. Localio et al. [12] advocate the combined abdominosacral approach for the removal of large retrorectal tumors in adults. The benefits of the combined abdominosacral approach include improved visualization of structures, such as the ureters and the rectum itself via the anterior incision, as well as enhanced exposure of the nerve roots provided by the posterior approach. Also, this approach permits good vascular control and provides good exposure for wide resection.
Recently, some reports of a laparoscopic approach for retrorectal tumors has been published [13-15]. They demonstrated that the laparoscopic approach had major benefits of smaller wound, less postoperative pain and facilitated excellent visualization with precise dissection in a limited space between the tumor and neighboring structures. In the present study, we performed laparoscopic surgery in three patients who underwent an anterior approach. Three patients underwent total laparoscopic resection successfully. We performed the laparoscopic resection using five ports without any difficulty. And the specimen was removed through the additional Pfannenstiel skin incision. One patient underwent a combined approach that, after the upper extent dissection and mobilization of the tumor through the laparoscopic abdominal approach on patient's supine position, the lower extent dissection and removal of the tumor was performed through the posterior approach on the patient's prone position. In this case, we performed the laparoscopic dissection and mobilization without any difficulty and verified the virtue that an additional abdominal incision for removal of the tumor can be avoided. As shown in Table 2, there was no postoperative complication in patients who underwent the laparoscopic abdominal approach. Also, laparoscopic surgery had a positive tendency in the aspect of postoperative recovery. Recently, surgeons have become familiar with the pelvic anatomy by the accumulation of experience in laparoscopic rectal surgery. Also, the laparoscopic approach has a virtue of an avoidance of large abdominal skin incision. Based on these finding, we expect that the laparoscopic approach may be a meaningful method in abdominal approach for the resection of benign retrorectal tumor. Especially, a laparoscopic approach with combined approach for large tumors benign in nature in preoperative imaging tests may have considerable merit.
In conclusion, although the retrorectal tumor is an uncommon disease, maintaining a high index of suspicion is the most important factor in early diagnosis. Exact understanding of the anatomy for the retrorectal region and the application of a proper diagnostic tool are important not only for the diagnosis but also the establishment of a treatment plan. Complete surgical resection with negative margin is recommended to relieve pressure symptoms and to provide a definitive diagnosis. Also, laparoscopic surgery in an abdominal approach may not only offer an excellent visualization of the deep structures in the retrorectal space but also reduce surgical trauma and provide earlier recovery.

 XML Download
XML Download