

 Citation
Citation Print
Print


INTRODUCTION
Primary segmental volvulus (PSV) of the ileum is a rare type of small intestinal volvulus, which is defined as the abnormal twisting of a loop of bowel around the axis of its own mesentery. It is considered a surgical emergency in neonates because of the high rates of small bowel necrosis or perforation leading to increased morbidity and mortality. Herein, we report a case of PSV of the ileum whose clinical features seemingly appeared to be meconium plug syndrome.
CASE REPORT
A 2-day-old female neonate weighing 2,210-g was referred to a pediatric surgeon because of abdominal distension and failure to pass meconium since birth. The baby was delivered by cesarean section due to premature rupture of membrane at 33+6 weeks' gestation. The Apgar scores were 8 at 1 minute and 9 at 5 minutes.
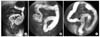
The infant showed progressive abdominal distension with an event of a small amount of bilious vomiting and could not pass meconium within 48 hours after birth. Initial simple abdominal films showed multiple dilated small bowel loops suggesting lower gastrointestinal obstruction. Contrast enema with gastrografin performed on the 3rd day demonstrated multiple filling defects throughout the entire colon and the rectum (Fig. 1A, B). Despite meconium plug evacuation by contrast enema, the abdomen remained distended. Rectal suction biopsy, which was executed the following day to rule out Hirschsprung's disease, showed negative for acetylcholinestrase immunohistochemistry. At the 5th day, another contrast enema was performed due to progressive abdominal distension and showed scant meconium plugs in the colon but a 'bird-beak' -like filling defect in the terminal ileum (Fig. 1C).
At the explorative laparotomy under the working diagnosis of partial ileal obstruction, a 25-cm long ileum, 2 cm proximal to the ileocecal valve, was twisted with pregangrenous state but not perforated (Fig. 2A). Both proximal and distal knots of the intestinal wall were paper-thin, nearly perforated (Fig. 2B). The lumen was almost atretic but maintained its own continuity. End-to-oblique anastomosis was performed after resection of ischemic ileal segment. The ligament of Treitz was located left of the vertebra with cecum in the right lower portion. The patient was discharged 11 days after operation without any complication. The patient is currently 2 years old and doing well.
DISCUSSION
Volvulus without malrotation is very rare and generally carries a high rate of mortality. PSV is torsion of a segment of the small intestine without any other abnormalities such as malrotation, congenital bands, postoperative adhesions, duplication cysts, or Meckel's diverticulum [1-3]. Some studies suggest that volvulus without malrotation occurs in 19 to 26% of small bowel volvulus, however, PSV of the ileum during the neonatal period is extremely rare [1,4].
Distension and increased peristalsis are considered to form a primary loop and twist the bowel [5].
Like other late intrauterine mesenteric vascular insults such as midgut volvulus, intussusceptions and internal hernia, PSV can lead to vascular insufficiency and cause ileal atresia [6,7]. It is thought that if the baby had been born at full term, this PSV might have resulted in ileal atresia with or without meconium peritonitis.
Early diagnosis of PSV is difficult because of its rarity and non-specific intestinal obstructive symptoms such as abdominal distension, bilious emesis or failure to pass meconium. We initially misdiagnosed this case as meconium plug syndrome because of the clinical features, radiologic findings of the contrast enema with impacted meconium plugs throughout the entire colon and rectum. Meconium plug syndrome is a transient disorder and is not associated with other intestinal abnormalities. In some instances, Hirschsprung's disease, cystic fibrosis or small left colon syndrome may present as meconium plug syndrome [8]. Hirschsprung's disease was ruled out in this case by rectal suction biopsy at the 4th postnatal day. Repeat contrast study or abdominal computed tomography scan can be beneficial to an accurate diagnosis [9]. The 'bird-beak' appearance in the second contrast enema in the current case, which implicates a knot in the distal intestine, was an important clue to diagnose PSV of the terminal ileum, in retrospect.
Clinical course of PSV of the ileum can be catastrophic, with a complete obstruction, massive passage of rectal bleeding in some cases consequently causing intractable shock state [10]. Compared to volvulus with malrotation, the ischemic changes of PSV progress suddenly because the colon, which plays the role of a cushion, is not involved. Ninety percent has ischemic changes and 40% perforations were observed in PSV compared to only 15% bowel strangulations in volvulus with malrotation [1]. Thus, PSV of the ileum is considered as an urgent surgical disease and therefore surgeons' timely and proper decision to perform an emergency operation is imperative.
In summary, we report a very rare case of PSV of the ileum in a neonate, whose manifestations were initially similar to those of meconium plug syndrome. We suggest PSV of the ileum should be considered as one of the underlying causes of neonatal colonic obstruction if meconium plug syndrome is not improved.

 XML Download
XML Download