

 Citation
Citation Print
Print



INTRODUCTION
Pneumatosis intestinalis (PI) is a rare and unexpected disorder defined as accumulation of gas in the submucosa or subserosa of the large or small intestine. It is associated with a variety of diseases, and its pathogenesis is still obscure. PI is an infrequent complication of liver transplantation (LT). Until now, it has been reported in 12 cases after pediatric orthotopic LT [1-5], although nearly none has been reported in adult liver recipients.
We report three cases of adult liver transplant recipients in whom the diagnosis of PI was made by computer tomography (CT) and simple X-ray (Table 1).
CASE REPORT
The patients in case 1 and 2 were unremarkable during post-operative period, and they were discharged home. The patient in case 1 experienced high fever and watery diarrhea after two months and the patient in case 2 complained of watery diarrhea after four months. The patient in case 3 experienced high fever and watery diarrhea one month after the transplantation without discharge. At admission, all patients were stable in blood pressure, pulse rate, and respiratory rate, but in case 1 and 3, patients had high body temperature (38.8℃ and 38.5℃).
The physical examination showed severely distended, non-tender abdomen, with hypoactive bowel sound and tympanic percussion in case 1. Other patients showed no specific findings. The laboratory findings of all cases did not reveal abnormal findings except mildly elevated C-reactive protein, ranging 0.38 to 1.59 mg/dL (normal range, <0.3 mg/dL). Serial blood tests of case 1 were positive twice for cytomegalovirus (CMV) antigenemia, but other cases showed all negative results. The peak titer of CMV antigenemia was 10/400,000 and colonoscopic finding did not show abnormal finding in case 1. The cytotoxicity assay of the all patient's stool was negative for Clostridium difficile toxin. Stool cultures and special stains for micro-organisms were all negative in all patients. The work-up failed to demonstrate an infectious etiology for the gastrointestinal symptom.
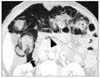
Abdomen simple X-rays and CT in abdomen revealed diffuse pneumatosis intestinalis of the colon, ileus, and free air under diaphragm, but no air in the portal vein in case 1 and 2 (Fig. 1). An abdominal CT of case 3 demonstrated pneumopericardium, diffuse linear pneumatosis intestinalis of the colon and extraluminal air within retroperitoneum and mesentery but no free intraperitoneal air (Figs. 2, 3).
All patients were conservatively managed with bowel rest, parenteral nutritional support, intravenous antibiotics (cefotaxime, ampicillin/sulbactam, and metronidazole) because of no signs of peritonitis. The patients in case 1 was treated with additional antiviral agent (ganciclovir) for positive CMV antigenemia and nasogastric tube decompression for free air, but other patients did not receive antiviral agent and did not have nasogastric tube decompression. The patients in case 1 and 3 did not receive immunosuppressive agent for 1 week, but the patient in case 2 received reduced immunosuppressive treatment with FK506 (2 mg daily), methylprednisolone (2 mg daily), and mycophenolate mofetil (500 mg daily). He remained in excellent general condition from the admission and had a sense of well-being during hospitalization.
The abdominal distension of case 1 resolved and diarrhea improved within a week and antibiotics were discontinued. All patients were given a diet, and were discharged home after the PI resolved clinically and radiographically.
DISCUSSION
The common factor linking PI to organ transplant recipients is steroid treatment [6]. In this report, one patient did not receive steroid treatment and the other two had steroid treatment but the amount was only 4 mg/day. Drug concentrations of FK506 and mycophenolate mofetil (MMF) in all patients have low levels as well. It might be possible that immunosuppression including FK506, steroid, and MMF did not cause of PI in our cases.
Symptoms that have been attributed to PI are in decreasing order of frequency: diarrhea, bloody stool, abdominal pain, abdominal distension, constipation, weight loss, and tenesmus [7]. In this report, three recipients had watery diarrhea, and two had high fever.
The physical examination of recipients did not show specific findings except abdominal distension in one case. The patients did not have abdominal pain, tenderness, rebound tenderness, and rigidity of abdominal wall. There was no clear evidence of peritonitis despite of pneumoperitoneum and air density in mesentery and retroperitoneum in simple X-rays and CT scan of abdomen. We assumed that there was no direct communication between lumen and peritoneum, therefore conservative treatment should be performed rather than surgical exploration. PI improved spontaneously after nearly one week of bowel rest and antibiotic therapy.
However, patients with white blood cells of more than 12,000/mm3 with or without the symptoms of clinical obstruction such as emesis, vomiting, and pain, age over 60 years were considered to be candidates for surgical intervention [8].
Based on this report, PI should be considered as the differential diagnosis of adult after LT who suffers from watery diarrhea and fever. Pneumoperitoneum, air-density in mesentery and retroperitoneum in patients with pneumatosis intestinalis without signs of peritonitis improved with conservative management.



 XML Download
XML Download