

 Citation
Citation Print
Print


INTRODUCTION
Sarcomatoid carcinoma is a rare histopathological entity with uncertain histogenesis that is composed of mixed carcinoma cells and mesenchymal cells. It is known to occur in various organs, but is most common in the head and neck, lung, and female genital tract [1]. Sometimes it arises in the gastrointestinal tract, predominantly in the esophagus or the stomach [2,3]. Colonic sarcomatoid carcinomas are rare tumors, with 22 cases documented either as sarcomatoid carcinomas or carcinosarcomas in the literature [4-25]. This tumor is generally aggressive with a poor prognosis. Here, we present a case of sarcomatoid carcinoma in the sigmoid colon which was extremely aggressive.
CASE REPORT
A 59-year-old man who had no significant past medical history was presented to the hospital with lower abdominal pain and discomfort which had begun 2 weeks earlier. Physical examination revealed a nontender, fetal-head-sized hard mass on palpation of the lower abdomen. Laboratory evaluation revealed anemia (9.5 g/dL) with elevated serum levels of carcinoembryonic antigen and carbohydrate antigen 19-9 (13.59 ng/mL, 56.07 U/mL).
Abdominal sonogram showed a large mass in the pelvic cavity with ascites and a metastatic liver nodule in S8.
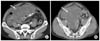
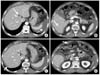
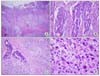
One day after admission, the patient complained of severe abdominal pain, and the serum hemoglobin level decreased to 7.15 g/dL. Computed tomography (CT) showed a ruptured 14 × 15 × 12 cm sized heterogenous low density mass in the pelvic cavity with fluid collection (Fig. 1), and there were multiple liver nodules and an enhanced nodule with fat infiltration in the omentum (Fig. 2). Urgent laparotomy was performed and multiple liver metastases and peritoneal and omental seeding of the tumor were found. The mass originated from the sigmoid colon. Sigmoid colectomy and tumorectomy were performed with an end colostomy for survival. Worsening abdominal distension and vomiting occurred 10 days after operation, and a repeat CT showed a 10 × 13 cm sized new mass in the pelvic cavity with small bowel obstruction. Repeat laparotomy was performed for palliative cytoreductive treatment, with small bowel resection and end ileostomy with debulking. The patient tolerated a slight advance in diet after the second surgery for three days, but ultimately abdominal distension recurred with a hard palpable mass, and the patient died of abdominal compartment syndrome due to rapid tumor growth 22 days after the initial operation. Histologic examination revealed an invasive tumor with two components: the luminal surface of the tumor was mainly composed of moderately differentiated adenocarcinoma, and in the deeper area there were spindle and epithelioid cells showing high grade anaplasia, which morphologically corresponded to the sarcoma (Fig. 3). The immunohistochemical study showed pancytokeratin expression in the adenocarcinoma component. The sarcomatous cells were focally positive for vimentin and cytokeratin (Fig. 4). A few variable tumor nodules were seen in the separately sent mesentery and omentum. They consisted mostly of the sarcomatous component. Five of eight lymph nodes isolated in the pericolic fat were positive for tumor metastasis.
DISCUSSION
Sarcomatoid carcinoma is widely considered a rare, highly aggressive tumor which arises most commonly in the head and neck or female genital tract [1]. It sometimes involves the upper aerodigestive tract such as the stomach and esophagus, and most have polypoid growth patterns and can be diagnosed early in their course, so are associated with a relatively favorable prognosis. However, since the time that Weidner and Zekan [4] reported the first case of colonic sarcomatoid carcinoma, most sarcomatoid carcinomas of the colon have been found to have an aggressive clinical course, often presenting with symptoms or signs related to distant metastasis.
To our knowledge, there have been 22 cases of colon carcinosarcomas and sarcomatoid carcinomas reported in the literature [4-25], and are summarized in Table 1. Mean age of diagnosis was 63.70 ± 17.64 years (male, 71.78 ± 10.79; female, 58.50 ± 19.51) with an age range of 13 to 86 years. Eighteen patients (78%) have metastasis with the liver being the most common location. There were 5 cases of right side colon (cecum and ascending colon), 2 cases of transverse colon, 5 cases of left side colon, and 11 cases (48%) of sigmoid colon and rectal sarcomatoid carcinoma. The prognosis is poor, with patients dying within 6 months of diagnosis in 13 (56%) of 23 cases. The longest published survival has been 49 months after initial diagnosis [4].
The histogenesis of sarcomatoid carcinoma is controversial. Morphologically, the presence of distinct carcinomatous and sarcomatous components suggests a different origin. However, the molecular analysis perfomed in the current case supports the hypothesis of a common cell precursor since the same mutation (R282W in exon 8 of the p53 gene) and the same allelic status (with the loss of 18q21) were identified in both the carcinomatous and sarcomatous components.
It is known that lymph nodes and distant metastases show a predominance of the carcinomatous component, and only one case has been documented that shows metastasis with the sarcomatous component [13].
There are no specific treatment guidelines due to the limited number of cases of colonic sarcomatoid carcinoma, however, radical surgery with adjuvant chemotherapy and close follow-up may be an acceptable approach to this disease [15].
In this case, our patient unfortunately had no chance for adjuvant chemotherapy. Despite two operations, the patient did not survive past 22 days due to rapid tumor growth. The present case may be the most aggressive case of colonic sarcomatoid carcinoma reported so far.


 XML Download
XML Download