

 Citation
Citation Print
Print


INTRODUCTION
Mucoceles of the appendix are uncommon, accounting for only 0.2 to 0.3% of appendectomy specimens [1]. An appendiceal mucocele is a cystic dilatation of the appendiceal lumen by accumulation of mucus, and may include mucosal hyperplasia, a mucinous cystadenoma, or a mucinous cystadenocarcinoma [2]. Frequently, the diagnosis of an appendiceal mucocele is made post-operatively because the manifestations are similar to appendicitis.
Laparoscopic appendectomy is widely used for the treatment of appendicitis, but laparoscopic resection of appendiceal mucoceles is not routine. We recently managed two large appendiceal mucoceles by laparoscopic resection and report our technique herein.
CASE REPORTS
Case 1
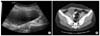
A 44-year-old woman sought evaluation from a gynecologist for a palpable right lower quadrant mass. The abdominal mass was found incidentally while bathing 2 months ago, and has persisted. The physical examination revealed a smooth, mobile mass in the right lower quadrant. She underwent a laparoscopic tubal ligation for contraceptive purposes 20 years ago. The blood chemistries and other laboratory findings were normal. A computed tomography (CT) scan and ultrasonography of the abdomen showed a 14 × 5 × 4.5 cm cystic mass arising from the cecum (Fig. 1). The patient was referred to the department of general surgery, where we discussed the surgical options and recommended a laparoscopic resection.
Case 2
An 81-year-old man had a palpable right lower quadrant mass of 2 months duration and severe headaches. Brain and abdominal CT scans revealed a chronic subdural hematoma and a large, tubular, cystic appendiceal mucocele, 15 × 4.5 × 4 cm in size. A colonoscopy also demonstrated a large protruding mass from the cecum (Fig. 2A). After evacuation of the subdural hematoma, a laparoscopic mucocelectomy was performed 1 month later.
Procedure
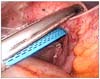
Because the laparoscopic procedure for cases 1 and 2 was similar, only case 1 is presented in detail. After the induction of general anesthesia, a 10-mm trocar was placed through a supraumbilical incision using the open Hasson technique because of the previous infraumbilical incision for the laparoscopic tubal ligation. A pneumoperitoneum was made by insufflation of carbon dioxide through the supraumbilical trocar to a pressure of 13 mmHg. One 12-mm trocar for the primary surgeon was inserted in the left lower quadrant of the abdomen. A freely-movable, sausage-shaped mass originating from the cecum was identified through the laparoscope. A 10-mm suprapubic trocar was inserted for retraction of the mucocele during the dissection and for extraction of the specimen (Fig. 3). To clear the small intestine from the surgical field, the patient was placed in the left decubitus and reverse Trendelenberg position. A laparoscopic bag was used for handling the mucocele because the surface of the mucocele was too slippery and tense to grasp. The primary surgeon manipulated the mucocele with the use of gravity and the laparoscopic bag wrapping the body of the mucocele, thereby reducing the risk of perforation and possible intraperitoneal spillage of mucinous content (Fig. 4). Mobilization of the cecum from the lateral wall and division of the mesoappendix were performed using an ultrasurgical device (Harmonic Scalpel, Ethicon Endo-Surgery, Cincinnati, OH, USA). Because there was no segment of normal appendix, the base of the cecum was resected with the mucocele. Another instrument was needed to retract the ascending colon and terminal ileum during this procedure, thus another trocar site was placed in the right upper quadrant. The mucocele was moved to in the caudal direction by the laparoscopic bag, then an endoscopic stapling device (Multifire Endo GIA, 60 mm; US Surgical Co., Norwalk, CT, USA) was used to perform the partial resection of cecum. The specimen (Fig. 5) was extracted through the suprapubic incision extended from the suprapubic trocar site and sent to a histopathologist. Frozen and permanent histopathologic evaluations of the appendicial mucocele were reported as a mucinous cystadenoma. The patient's post-operative course was uneventful. A follow-up colonoscopy was performed, which showed no abnormal findings.
DISCUSSION
The neoplastic variety of a mucocele occurs from distention of the appendiceal lumen by mucus secreted from proliferating tumor cells. The benign form of a mucocele is a mucinous cystadenoma and the malignant form is a mucinous cystadenocarcinoma. These lesions secrete an excess of mucus while blocking outflow into the cecum, thus creating a distended appendix.
The pre-operative diagnosis of an appendiceal mucocele is difficult due to the non-specific nature of the findings. The classic clinical features of an obstructive appendiceal mucocele includes right lower quadrant discomfort, a palpable mass, and x-ray findings of a filling defect in the cecum with non-visualization of the appendix. On CT and ultrasonography, a nodular, enhancing lesion in the wall of the mucocele is suggestive of malignant disease [3]. Sometimes, it is asymptomatic and discovered incidentally at surgery or during imaging evaluation for another disease.
If a mucocele is found, therapy is surgical. The appropriate type of surgical treatment is related to the dimensions and the histology of the mucocele. An appendectomy is used for simple mucoceles or cystadenomas when the appendiceal base is intact. Cecal resection is indicated for cystadenomas with a large base, and a right hemicolectomy is recommended for cystadenocarcinomas. The 10-year survival of patients with mucinous cystadenocarcinomas is 65% among patients treated by hemicolectomy, but only 37% among patients treated by appendectomy alone [4].
While several cases of laparoscopic treatment of appendiceal mucoceles have been reported [4-8], many authors suggest that the laparoscopic approach should be avoided because of the increased risk of rupture and subsequent pseudomyxoma peritonei [9,10]. Pseudomyxoma peritonei is caused by spillage and implantation of mucin-secreting cells into the peritoneal cavity. Thus, we reasoned that the complication rate of pseudomyxoma peritonei during laparoscopic surgery would be the same as that of open surgery if a minimal-touch technique was utilized.
Lau et al. [6] reported the laparoscopic resection of a 12 cm large mucocele using gravity and position during minimal manipulation of the lesion. Navarra et al. [7] also reported successful laparoscopic resection of an appendiceal mucocele and suggested that conversion to a laparotomy should be considered if the lesion is grasped traumatically or if the tumor clearly extends beyond the appendix. Recently, Chiu et al. [8] presented a case involving the successful laparoscopic resection of an 8 cm appendiceal mucinous cystadenoma. González Moreno et al. [9] reported a case of an appendiceal mucinous tumor resected by laparoscopy associated with subsequent diffuse peritoneal carcinomatosis. They suggested that if distention of the appendiceal lumen is observed laparoscopically, suggesting a mucocele as a possible diagnosis, conversion to open appendectomy may be the most prudent surgical judgment. We performed laparoscopic resections of two appendiceal mucoceles using a laparoscopic bag to retain and retract the mucocele, in addition to using gravity and position, therefore we avoided grasping the tumor directly.
The application of laparoscopic surgery has been more widely adopted in the treatment of gastrointestinal diseases, and in some cases laparoscopic surgery is currently the standard treatment. In the surgical treatment of appendiceal mucoceles, however, open surgery is currently the standard surgical treatment due to its well-known safety and easy accessibility. The authors are also aware of the possibility of rupture during laparoscopic dissection, and the subsequent fatal complication of pseudomyxoma peritonei. Nevertheless, if we can handle the tissue with minimal manipulation, and can secure enough safety by using various laparoscopic instruments, laparoscopic resection of an appendiceal mucocele might be an alternative surgical option to open surgery.



 XML Download
XML Download