

 Citation
Citation Print
Print


INTRODUCTION
Perforation is a complication of diverticulosis that requires an urgent operation. Depending on the location of the perforation, signs of peritoneal irritation may be evident in cases of intra-peritoneal free perforation but hidden in cases of retroperitoneal perforation. The abscess or colonic gas may spread via various anatomic pathway when perforation of diverticulitis in the retroperitoneum occurs, and diverse atypical clinical symptoms may be present [1]. Thus, the atypical manifestation of retroperitoneal perforation of diverticulitis can cause difficulties when making the diagnosis. The delayed diagnosis and treatment could result in high morbidity and mortality. Pneumomediastinum is initiated by many precipitating factors or diseases [2]. However, it is rarely associated with colonic perforation, particularly in patients with no history of colonoscopic procedure [3-6]. Here, we report a case of pneumomediastinum caused by retroperitoneal colonic diverticulitis perforation.
CASE REPORT
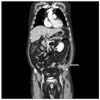
A 59-year-old man was referred to the emergency department because of persistent abdominal and left flank pain. He had no specific past medical history. The left flank pain had started 30 days before this visit as an acute nephrolithiasis. He had visited the local clinic and presumptive impression was left ureter stone because left costovertebral angle (CVA) tenderness was apparent although radiologic study was not performed. Thus, he had received conservative management such as analgesics for pain control. However, the left flank pain worsened and was accompanied by abdominal pain 1 week ago. On physical examination, the patient looked ill and had a temperature of 38.2℃, the blood pressure was 90/40 mmHg, the pulse rate was 101 beats/min, and the respiratory rate was 24 breaths/min. The abdomen was slightly distended and tender over the lower abdomen, without signs of generalized peritoneal irritation. However, left CVA tenderness was apparent. Laboratory results were within the normal range, except for the white blood cell count of 21,000/µL. Chest x-ray showed scanty bilateral pleural effusion without pneumomediastinum or free air in the peritoneal cavity (Fig. 1). There were no specific findings in the simple abdomen (Fig. 2). However, a computed tomography scan showed an infiltrative mass in the descending colon involving the left para-renal space. In addition, it showed massive air bubbles in the left retroperitoneum with diffuse infiltrates into the soft tissue (Fig. 3) and a pneumomediastinum (Fig. 4). An emergency operation was performed because of suspected diverticulitis or colon cancer perforation with abscess formation. During the operation, a colonic diverticulitis perforation over the posterior wall of the sigmoid descending junction and a retroperitoneal abscess with necrosis of the parietal peritoneum were found. Crepitation could be felt starting from the left retroperitoneum up to the diaphragm. The abscess was evacuated, and the necrotic tissue was resected. A segmental resection of the diseased colon and end colostomy were performed (Hartmann's procedure). Post-operative culture of the drain revealed Enterococcus faecalis, which were sensitive to various antibiotics including penicillin, vancomycin, erythromycin, ciprofloxacin, and gentamicin. Thus, we added vancomycin instead of metronidazole to the previous empirical antibiotics (1st generation cephalosporin, gentamicin, metronidazole) on the 4th post-operative day. However, the condition of the patient deteriorated progressively after operation. He died of sepsis and multiorgan failure on the 5th postoperative day.
DISCUSSION
Colonic diverticulosis is a common disease, and its incidence increases with aging. Among the patients with colonic diverticulosis, approximately 20% may develop diverticulitis as a result of infection and inflammation of the diverticuli [7]. The complications of diverticulitis are stricture, bleeding, perforation, and fistula formation. The perforation of diverticulitis is one of the most serious complications that require an urgent operation. The perforated lesion is usually covered and leads to abscess formation, whereas free perforation into the peritoneal cavity leading to diffuse peritonitis is relatively rare [8]. In cases of free perforation, an early diagnosis could be possible because the peritoneal irritation sign is evident. The diagnosis of diverticulitis perforation may be difficult depending on the location of the perforation, e.g., perforation into the retroperitoneal space. In such cases, its manifestation can be presented with various conditions, including thrombophlebitis of the leg, inguinal abscess, hip and buttock pain, subcutaneous emphysema, and shortness of breath [1,3-6].
These various pathologic conditions caused by diverticulitis perforation can be explained by considering the anatomy. Meyers [9] reported that if gas is present in the para-renal space, which can be caused by sigmoid diverticulitis perforation, its progression from the posterior para-renal space through the diaphragm hiatus results in pneumomediastinum and cervical subcutaneous emphysema. Maunder et al. [10] reported that the soft tissue compartment of the neck, thorax, and abdomen contains four regions defined as the subcutaneous tissue, prevertebral tissue, visceral space, and previsceral space. The visceral space extends from the neck through the mediastinum to the retroperitoneum, forming an anatomic connection between these areas. Therefore, an abscess or colonic luminal gas caused by diverticulitis perforation into the retroperitoneal space can spread to the other areas, resulting in unusual manifestations, similar to those observed in our case.
The unusual complications of diverticulitis perforation have been reported, e.g., subcutaneous emphysema, cellulitis, necrotising fasciitis, pneumopericardium, pericarditis, pneumothorax, and pneumomediastinum [1,3-6]. Pneumomediastinum is a condition in which air is present in the mediastinum. It can be caused by traumatic injury, intrathoracic infections, excessive coughing, sneezing, and in rare cases, colonic perforation, which is associated with a complicated colonoscopic procedure [2]. To the best of our knowledge, there have been 5 cases of pneumomediastinum as a sequence of diverticulitis perforation in English literature (Table 1). In these cases, the main symptoms were abdominal pain and fever, which were often accompanied with subcutaneous emphysema [3-6]. The symptoms and clinical signs of retroperitoneal diverticulitis perforation may be unclear and nonspecific at an early stage, and complications may occur without any previous symptoms of diverticulitis. Therefore, making the correct diagnosis could be delayed and difficult, like in our case [4].
In concusion, pneumomediastinum caused by retroperitoneal diverticulitis perforation is a very rare manifestation, and the symptoms are unclear. This leads to a delayed diagnosis, which can cause a life-threatening condition, particularly in patients without signs of peritonitis. It is necessary to consider the possibility of a colonic origin in patients presenting with abdominal pain and showing findings of pneumomediastinum for the prompt management of this condition.




 XML Download
XML Download