

 Citation
Citation Print
Print


INTRODUCTION
By using DNA microarray techniques, it has been shown that breast cancers can be classified into biologically distinct groups based on their gene expression profiles. These groups comprise luminal A (estrogen receptor [ER]-positive and human epidermal growth factor receptor-2 [HER2]-negative), luminal B (ER- and HER2-positive), HER2 (ER-negative and HER2-positive), and triple negative (ER- and HER2-negative) subtypes [1,2]. The TNBC is a heterogeneous group and is further categorized into the basal-like and the normal breast subtypes, which are positive and negative, respectively, for myoepithelial/basal markers such as basal cytokeratins (CKs) (i.e., CK5/6, CK14, and CK17), a-smooth muscle actin, and epidermal growth factor receptor (EGFR) [3,4]. Although TNBCs account for only 10 to 17% of all breast carcinomas, this subgroup is regarded as important clinically because of the aggressive clinical behavior, poorer patient prognosis, and lack of an established therapeutic target [5,6]. The ratio of basal-like subtype in TNBC was estimated to be up to 56 to 84%. Therefore, characteristic histopathological features of TNBCs are similar with those of the basal- like subtype [7,8]. Characteristic histopathological types that constitute TNBCs and basal-like subtype are high-grade invasive ductal carcinoma of no special type, typical medullary carcinoma, metaplastic carcinomas, and adenoid cystic carcinoma [1,9]. So we present data of histological features of TNBCs and discuss about its morphological spectrum in our hospital case.
METHODS
Patients and tissue samples
Tissue samples were obtained from 618 patients with invasive breast cancer who were diagnosed from 2000 to 2005 at Kosin University Gospel Hospital in Busan, Korea. A total of 618 specimens of primary invasive carcinoma were obtained from resected tumor. None of these cancer patients received treatment prior to surgery. The patients underwent standard and partial mastectomies with fully resected axillary dissections. Patients received anthracycline- containing chemotherapy if the tumor was node positive. Endocrine therapy was given for 5 years to patients with ER-positive tumors. Median follow-up was 5.5 years (range, 0.3 to 14.8 years), during which there were 84 relapses and 32 deaths.
Immunohistochemical techniques
The expression of ER, progesterone receptor, HER2, CK5/6 and other biological markers was determined immunohistochemically in paraffin-embedded tissue specimens. Table 1 summarizes all the antibodies, dilutions, incubation times, and cutoff values used for this analysis. All data were collected from the pathology reports. Histopathological features such as hormone receptor status and HER2/neu status on immunohistochemistry (Dako, Copenhagen, Denmark) were all analyzed at the Institute of Pathology at the Kosin University Gospel Hospital. Expressions of p53, ERa, Ki-67, and ErbB2 were determined immunohistochemically on paraffin sections using antibodies against ERa (Dako), Ki67 (Dako), ErbB2 (Dako), p53 (Dako). Tumor necrosis was defined as the presence of necrosis of any dimension in a section of invasive cancer. Histologic grading was performed using the criteria of Bloom and Richardson. Lymphatic vascular invasion was defined as the presence of tumor emboli in peritumoral lymphatic spaces, capillaries or postcapillary venules. ER status and progesterone receptor status were taken as positive if more than 10% of tumor cells showed staining. Immunohistochemical score of 3+ or fluorescence in situ hybridization+ for HER2 was accepted as HER2 positivity.
Statistical analysis
Statistical tests were performed using the SPSS ver. 12.0 (SPSS Inc., Chicago, IL, USA). The survival function was calculated from the time of the pathologic diagnosis to the occurrence of death. Survival data were censored on December 31, 2009, which was the date on which the survival data were correlated with the death registry for the last time or 5 years after the onset of the disease. Kaplan-Meier estimates are presented for the survival function, and differences in survival were analyzed using the log rank test. Associations between specific histopathological and clinical survival estimates and curves were established using the Kaplan-Meier method and differences in observed survival distribution among patient subgroups were tested with two-sided log-rank test. All survival rates were presented with their standard errors. We used Pearson's correlation to determine the association of pairs of explanatory variables and differences in qualitative variables were evaluated by chi-squared test, where necessary. All P-values were two-sided and a P-value of less than 0.05 was considered to indicate a statistically significant difference.
RESULTS
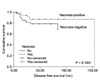
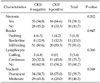
The main clinicopathological characteristics of the patients in our series are summarized in Table 2. Mean age was 54 years. Luminal A was reported in 166 patients (26.9%). Luminal B, HER2 and triple negative type was reported in 178 patients (28.9%), 162 patients (26.3%), 111 patients (17.9%), respectively. Among the 111 TNBC patients, twenty four had missing data as a result of a computer failure, so that 87 TNBC patients are included in the final morphologic characteristics data set. Other reasons for ineligibility included incompetent specimen. Tumor necrosis was found in 51 patients (58.3%) in TNBC. And infiltrating border was found in 71 patients (81.0%). Also continuous lymphocytic distribution and prominent nucleoli was found in 31 patients (35.7%), 52 patients (59.7%), respectively. No association was detected between pathologic characteristics and other biological markers (Table 3). Among TNBC patients, 87 patients could be studied about CK5/6. According to the positivity of CK5/6, 24 of the 87 patients (27.6%) had been diagnosed as CK5/6 (+) TNBC and 63 patients (72.4%) had CK5/6 (-) TNBC (Table 4). No statistical relationship was found between CK5/6 positivity and the other variables, such as tumor size, nodal status, American Joint Committee on Cancer stage, tumor grading, p53 and Ki67. Tumor necrosis was found in 16 patients (66.6%) in CK5/6 (+) TNBC. And infiltrating border was found in 20 patients (83.3%) in CK5/6 (+) TNBC. Also continuous lymphocytic distribution and prominent nucleoli was found in 20 patients (32.2%), 34 patients (54.7%) in CK5/6 (-) TNBC respectively. But there is no significant association between CK5/6 (+) TNBC and morphologic characteristics (Table 4, Fig. 1). At a median follow-up of 5.5 years, 84 patients (13.6%) had a recurrence. And 32 patients (5.2%) had a death. Among TNBC, we observed 11 relapses in 63 patients (17.5%) with CK5/6 (-) TNBC and only 1 relaps in 24 patients (4.1%) with CK5/6 (+) TNBC. Disease-free survivals was not shorter in patients with CK5/6 (+) TNBC at diagnosis when compared with patients with CK5/6 (-) TNBC (hazard ratio [HR], 0.371; 95% confidence interval [CI], 0.047 to 2.922; P = 0.3257). Also overall survival was not shorter in patients with CK5/6 (+) TNBC (HR, 0.786; 95% CI, 0.327 to 6.879; P = 0.2752) (Table 5).
DISCUSSION
Among the high-grade invasive ductal carcinomas, a large part of cases is made up of high-grade solid-tubular carcinoma (also called as atypical medullary carcinoma) [1,10]. Typical medullary carcinoma is defined as a well-circumscribed carcinoma composed of poorly differentiated cells arranged in large sheets syncytial architecture with scant stroma, with no glandular structures, and with a prominent lymphoplasmacytic infiltratation, and with a pushing border of invasion [11,12]. Central geographic or comedo-type necrosis may also be seen. Tumors showing the association of a predominantly syncytial architecture with only two or three of the other above-mentioned criteria are designated as atypical medullary carcinoma [13,14]. High-grade invasive ductal carcinoma with a large central acellular zone is also found relatively frequently in TNBCs. The independent prognostic significance of tumor necrosis has been studied extensively [15,16]. Controversy exists about the definition and classification of necrosis, with respect to the amount of necrosis that is considered to be significant as well as the relative distribution of necrosis within intraductal and invasive components of a tumor [17,18]. There is evidence indicating that the prognostic significance of tumor necrosis is time dependent. For example, Gilchrist et al. found that tumor necrosis defined as the "presence of confluent necrosis of any dimension in a section of invasive cancer that could be distinguished at intermediate magnification," was a significant predictor of time to recurrence and overall survival with 10-year follow-up [19,20]. And previous data add further support to the perception that extensive necrosis is a prognostically unfavorable feature in invasive mammary carcinoma, possibly reflecting a growth rate so rapid that it exceeds tumor sustaining angiogenesis to a substantial degree [21,22]. And the prognostic significance of stromal inflammatory cells within and around invasive duct carcinomas has been the subject of considerable interest and some controversy [23,24]. The reaction consists mainly of mature lymphocytes with a variable admixture of plasma cell, histiocytes, neutrophils, and mast cells. Rarely, plasma cells or eosinophils predominate. Tumors with plasma cell predominance are usually medullary carcinomas or carcinomas with medullary features [15,16]. The marked lymphoplasmacytic reaction observed in medullary carcinoma also occurs in a minority of non medullary invasive duct carcinomas [17,18].
In conclusion, these findings suggest that morphologic characteristics cannot be used to classify TNBC into at least two subtypes with differing prognoses. One of the reasons is that only a small number of patients were examined in this study, making it difficult to reach statistical significance. More abundant patients' date will be needed to evaluate of the morphologic characteristics' predictive role.




 XML Download
XML Download