

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Menopause is a natural biological process affecting the lives of all women.1 Following the increased life expectancy and the stabilization of menopause, women continue to live in the post-menopausal period about more than one-third of the rest of their lives; therefore, it is essential to maintain the welfare of women during this period as a top priority in preventing socioeconomical risks.234 A dramatic decline in both circulating estrogen and androgen levels with age during natural menopause period can render various sexual dysfunction, including little enthusiasm, poor arousal, dyspareunia, impaired orgasm and reduced satisfaction.5 The estrogen therapy may attenuate such impairments and improve urogenital atrophy sexual performance.678 In earlier times, one of the prevalent recommended remedies was hormone replacement therapy (HRT) to relieve the observed menopausal signs. Despite significant evidence of the benefits of HRT, common reportedly adverse effects such as cancer9 led to the switch to complementary and alternative medicine, including aromatherapy that is the practice of using extracted aromatic plant oils and materials through inhalation or oral and topical administration by bathing, compressing and massaging.91011 The therapeutic properties of this approach is through psychological and physiological (such as amygdala and hippocampus) routs.12 Previous investigations have shown the effectiveness of aromatherapy in healing sexual dysfunction in the menopausal women. Accordingly, the purpose of current systematic review and meta-analysis was to evaluate the effect of aromatherapy on relieving some sexual function.
Go to : 
Materials and Methods
The main study objective was to identify the effect of aromatherapy on sexual problem among menopausal women. The study was conducted on the published randomized controlled trials. The inclusion criteria were perimenopausal and postmenopausal women, study design of parallel or crossover groups, reported sexual symptoms and taking herbal medicines for aromatherapy. The searching process was done on the databases of MEDLINE, Scopus and the Cochrane Library (Cochrane Central Register of Controlled Trials) from inception to December 2017 regarding the trials on the effect of herbal medicines on the sleep disorders. It should be noted that the references mentioned in the searched articles were reviewed to search additional respective literatures. The keywords included (alternative medicine OR essential oils OR aromatherapy OR massage) and menopause in both English and Persian languages. Two reviewers separately assessed the quality assessment using Cochrane Collaboration's tool (Table 1) to check seven risks of bias, involving sequence generation, allocation concealment, structure of participants and personnel, structure of outcomes, incomplete data outcomes, selective reports and other sources of bias.

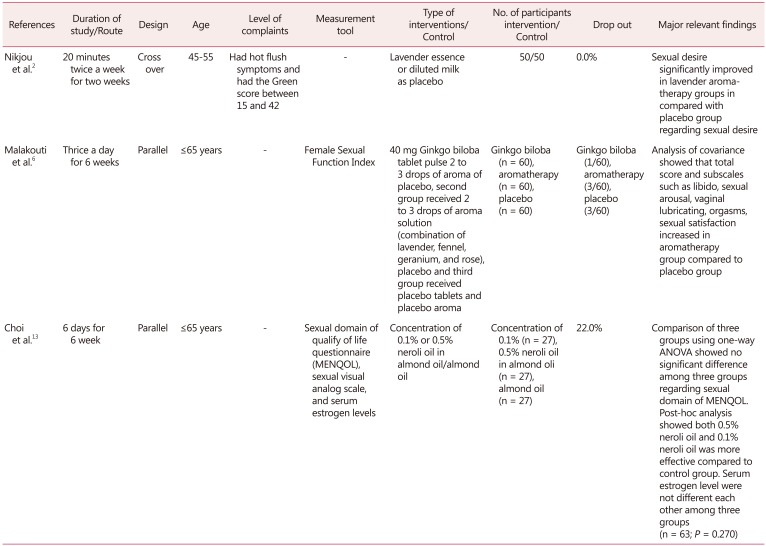
The data required for study were name of authors, name of country, design of study, range of age, status of menopause, level of complaints, type of measurement tool, features of intervention, number of participant in case and placebo group, rate of drop out and list of main outcomes. Table 2 showed characteristics of 3 randomized placebocontrolled trials included to systematic.
Standardized mean difference (SMD) was chosen for pooling finding from trials. The random effect model was used due to large high heterogeneity. The Cochrane Q and I2 index were applied to calculate the heterogeneity. Publication bias was not used due to small number of studies. All of mentioned analyses were conducted using comprehensive meta-analysis version 2 (Biostat, Englewood, NJ, USA).
Go to :
Results
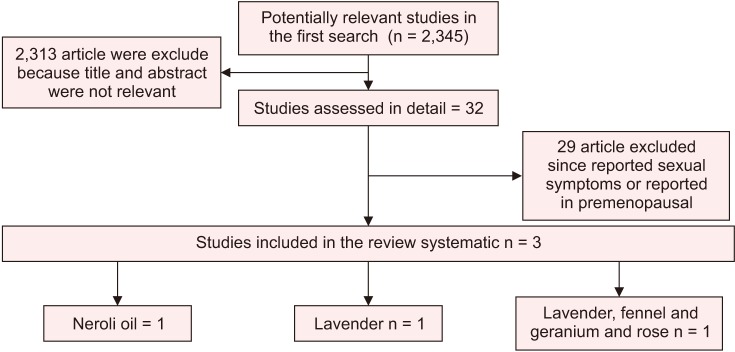
Process of selecting of included articles to systematic review (Fig. 1). Nikjou et al.2 conducted a crossover study and compared the effect of lavender aromatherapy (n = 50) with placebo (n = 50) on the sexual desire among the menopausal women, who suffered from hot flush symptoms with Green score of 15 to 42. The demographic profiles such as age, number of children, income adequacy and occupation were homogenous in both groups at baseline. First group received lavender and second group consumed placebo. After a 4-week wash out, the patients were switched to each other treatment for additional two weeks. The women were requested to smell bottle containing placebo or lavender for 20 minutes twice a week for two weeks. The sexual desire significantly was improved in the lavender aromatherapy groups as comparison with the placebo group (P < 0.001).
Malakouti et al.6 compared the effect of Ginkgo biloba tablet combined with aromatherapy inhaling on the sexual functions in post-menopausal women. Totally, 180 post menopause women were randomized into equally three groups. The Group I was administered 40 mg of Ginkgo biloba tablet along with 2 to 3 drops of placebo aroma. The Group II consumed 2 to 3 drops of aroma solution (a mixture of lavender, fennel, geranium and rose) and 40 mg of placebo tablet. The Group III used placebo tablets and placebo aroma. All treatments were administered thrice a day for 6 weeks. Female sexual function index (FSFI) was used to measure the sexual functions. A statistically significant difference was observed at baseline between two groups in total sexual score and its subscales, except for the severity of dyspareunia (P = 0.60). Also socio-demographical variables of age (P = 0.01), spouse job (P = 0.008), spouse educational level (P = 0.001), monthly income (P = 0.01), body mass index (BMI; P < 0.001), number of children (P < 0.001) and family size (P = 0.001). Lost to follow-up was three patients because of unwillingness to continue intervention in the aromatherapy group. Analysis of covariance (ANCOVA) with control for total sexual score and all subscales as well as control confounding variables such as number of children, family size, age and BMI were used to compare the groups. The ANCOVA results showed an increase in total score (P < 0.001) and subscales such as libido (P < 0.01), sexual arousal (P < 0.01), vaginal lubricating (P < 0.01), orgasms (P < 0.01), sexual satisfaction (P < 0.01) in the aromatherapy group (n = 57) compared to the placebo group (n = 57). Paired t-test used to pre- and post-tests was significant for the total score (P < 0.001) and all subscales of libido (P < 0.001), sexual arousal (P < 0.001), vaginal lubricant (P < 0.001), orgasm (P < 0.001) and sexual satisfaction (P < 0.001), except for dyspareunia (P = 0.24). In the placebo group, the difference in the pre- and post-tests was also significant for total score, libido sexual arousal and dyspareunia. Furthermore, 7% and 5.1% of the subjects in the intervention group reported skin redness and itching of forearm. The researchers reported no comparison between groups regarding the side effects of treatment. The satisfaction with treatment was estimated at 72.8% in the aromatherapy group.
Choi et al.13 compared the inhalation effect of essential oil from citrus auranitium L.var. amara on the sexual function dimensions of the menopause-specific qualify of life questionnaire (MENQOL) and sexual desire. A total of 81 menopausal women were divided into equally three groups. The first and second groups received respectively low dose (0.1%) and high dose (0.5%) of neroli oil, and the placebo group consumed the almond oil. The MENQOL is a self-reported 29-item questionnaire with 4 domains, including psychosocial,7 vasomotor domain,3 physical, and sexual function.3 The sexual desire was measured by visual analogue scale (VAS) with a 10-cm ruler ranged from zero (no sexual desire) to 10 (extremely strong sexual desire). The research units were requested to put a cross on the ruler at the point that the best represented intensity of sexual desire. Intergroup comparison using one-way analysis of variance (ANOVA) showed no significant difference between three groups regarding sexual domain of MENQOL. However, the sexual desire measured by VAS was different between the three groups. The ANOVA were followed by post hoc analysis and the results revealed that both low and high doses were more effective compared to the control group. The serum estrogen level were not different between the three groups (n = 63; P = 0.270).
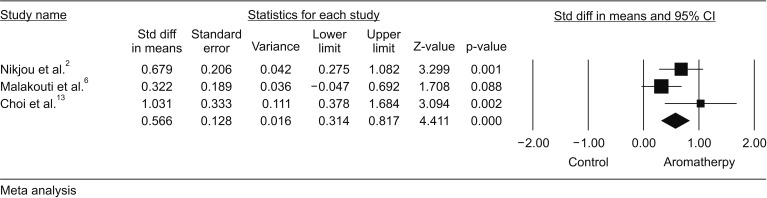
Three trials2613 had suitable data to include in the metaanalysis. Our meta-analysis showed that SMD of the sexual desire could be improved up to 0.5 in the aromatherapy group compared to the control group (SMD = 0.56; P < 0.001; heterogeneity; I2 = 42%; P = 0.141) (Fig. 2).
Go to :
Discussion
The present systematic review scrutinized the efficacy and safety of the aromatherapy on the sexual symptoms in the menopausal women. This systematic review detected three clinical trials, involving 225 menopause women. One of the herbal medicines included to this systematic review was lavender, and two measured outcomes were the sexual function and the estrogen serum levels. The inhalation of lavender improved significantly the sexual desire among the menopausal women suffering from hot flashes. The inhalation of Citrus auranitium L.var. amara improved the score of sexual desire as measured by VAS. However, it could not lead to significant changes regarding the sexual domain of MENQOL. The combined inhalation of lavender, fennel, geranium and rose was found to be more effective than in the control group on the total sexual score and the relevant subscales, except for dyspareunia. The serum estrogen level had no changes in two different doses in the neroli oil inhalation group than in the almond oil. Our meta-analysis showed a significant improvement in aromatherapy with phytoestrogens in the placebo group.
The aromatherapy via herbal essential oils occurs through different ways, including (1) inhaling the odor molecules (sense of smell) and sending impulses to the olfactory part of brain (which is linked to other controlling systems like memory, emotions, hormones, sexual feeling and heart rate) that trigger the release of hormones capable of stimulating, incubating, calming or creating euphoria absorption; (2) skin absorption of volatile oils and subsequently penetration into blood flow.
Choi et al.13 reported that the inhalation of neroli (at the concentrations of 1% and 0.5%) caused a statistically significant improvement in the sexual desire VAS score compared with the almond oil, whereas this significant change was not observed regarding score of sexual domain of MENQOL. The sexual domain of MENQOL consists of three items, including vaginal dryness, and two items related to sexual functions of “decrease in my sexual desire” and “avoiding intimacy”. Explained discrepancy between the results of two scale may related to this reason that the inhalation of oil are able to improve dimensions of sexual function such as sexual desire and intimacy but fail to improve subjective symptoms of vaginal dryness.
Although we think that our search strategy was comprehensive but it is possible to be failed to detect some studies. Only one trial used standardized and reliable tool to measure the sexual function. The use of standardized tool such as FSFI, Golombok-Rust inventory of sexual satisfaction - female version and the two-factor Italian McCoy female sexuality should be considered in future research regarding the effect of aromatherapy on the sexual function. Only one of the three trials reported the intention-to-treat (ITT) but there was no clean explanation of the adherence to treat. Three trials showed a significant effect on sexual function. However, further efforts are required to detect of the mechanism of action of aromatherapy with phytoestrogens on the sexual function. Only those trials assessing serum estrogen level and sexual hormones such as follicle-stimulating hormone, luteinizing hormone, sex hormone-binding globulin should be measured in future research.
Go to :
Conclusion
Aromatherapy with neroli oil or lavender (mono-preparation) and combined aromatherapy oils of lavender, fennel, geranium and rose significantly improved sexual function. However, there was no significant change in serum estrogen level. These findings should be presented cautiously because of limitations in this review such as lack of standardized tool, lack of reporting ITT, low number of studies and short-term follow-up.
Go to :
 XML Download
XML Download