

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Menopause is a physiological phenomenon caused by a decline in ovarian function1 and characterized mainly by amenorrhea and an end to fertility.23 Menopause normally occurs between 48 and 55 years of age and women live 30 or more years of their life at or around menopause. Menstruation stops in this period and women lose their fertility due to the reduced levels of ovarian hormones and pituitary gonadotropin.4
Passing through menopause and the changes in hormonal processes caused by it are associated with certain physical, psychological and sexual symptoms and complaints.56 The physical symptoms include hot flushes, vaginal atrophy, irritable bladder, palpitations, headache and muscle pain;7 the psychological symptoms include irritability, nervousness and depression; the sexual symptoms include a lack of sexual desire and decreased orgasm.8
These problems cause not only distress and disability, but also impose a burden on the limited healthcare resources available in countries.9 Understanding the pattern of these changes and the reasons for them is essential for women and helps them enter this stage of life less anxiously and with a more positive attitude.
Studies conducted in Iran on women's concern and attitudes toward menopause suggest that Iranian women consider menopause a biological phenomenon; however, entering new stages of life can be associated with different reactions depending on attitudes, beliefs, expectations and experiences.1011 As stipulated by Khademi and Cooke12 in a study on the role of sociocultural factors in both the physical and psychological symptoms of menopause, many factors affect this stage of women's life, including environmental factors, the socioeconomic status and the quality of health services. A review study by Martinez et al.13 on 51,410 urban and rural postmenopausal women revealed statistically significant differences between the two groups in terms of certain patterns of menopausal symptoms, as hot flushes, depression and joint pain were more severe in rural than in urban women. Malacara et al.14 also examined 7,632 postmenopausal women and found hot flushes to be more severe and vaginal dryness, dyspareunia and reduced sexual desire to be more common in rural than in urban women. The different severities of the symptoms were attributed to factors such as rural residence, low levels of education and a high body mass index (BMI).
Although hormonal changes and their subsequent problems are inevitable in this period, the severity of the symptoms can be controlled. Accepting menopause and having a positive attitude toward it can also help.15 Given the results of previous studies, and since environmental factors affect the pattern of menopausal symptoms and quality of life (QOL),16 and given that around one-third of the Iranian population lives in villages,17 the present study was conducted in North-West Iran to compare the pattern of menopausal symptoms, concern and attitudes in urban and rural postmenopausal women.
Materials and Methods
This cross-sectional study was conducted on urban and rural postmenopausal women residing in and around Tabriz, Iran, after obtaining the approval of the Ethics Committee of Tabriz University of Medical Sciences. The inclusion criteria consisted of a ceased menstruation for at least 12 months and five years at most, not having undergone any surgery within the past three months, the menopause being physiological and not using psychotropic medications. Unwillingness to participate in the study was the only exclusion criterion.
Sample size was estimated as 158 as per the study conducted by Hakimi et al.18 (m = 8.42 and standard deviation [SD] = 19.3) and with α = 0.05 and an accuracy of 0.1. Given the 1.5 effect size and a potential attrition of 15%, the minimum sample size was estimated as 544 overall and 272 per group.
Cluster sampling was used to select the subjects. A total of 46 clusters were assigned to the cities and 46 to the villages. A list of women aged 50 to 55 residing in Tabriz was obtained from the local National Organization for Civil Registration (extracted from the latest national census) and the home address of 46 of these women was randomly selected as the cluster heads.
To sample the rural subjects, a total of 23 villages were randomly selected from around Tabriz. Two clusters were randomly selected for each village using the census offices of the local health houses. In each cluster, six subjects from six families completed the questionnaire. Sampling began with the cluster head and continued sequentially to the left. The next house in line was visited in the case of the subject not meeting the inclusion criteria, being away from home or being unwilling to participate in the study. All the interviews were held by the first author and two other trained interviewers. After ensuring that they met the inclusion criteria, the participants were all asked to sign informed consent forms and were also ensured of their right to withdraw from the study at their own discretion.
The data collection tools used included a 13-item demographic questionnaire on personal details and a questionnaire to assess women's experiences during menopause. The score of menopausal experiences was obtained using a 44-item researcher-made questionnaire consisting of six subscales, including physical symptoms, psychological symptoms, concern, emotions, attitudes and adaptation to menopause. The psychometric assessment of the data collection tools was performed through examining their content and construct validity, internal consistency and test-retest reliability and by calculating their Cronbach's α (0.96) and Pearson's correlation coefficient (0.78).19
Both of questionnaires were completed for/by the participants through face-to-face interviews.
The data obtained from the questionnaires were analyzed in SPSS version 17.0 (SPSS Inc., Chicago, IL, USA). The level of statistical significance was set at P < 0.05. Descriptive statistics were used to describe the personal-demographic characteristics and menopausal symptoms. After adjusting the basic variables, including age, level of weducation, housing status, satisfaction with spouse's and children's behavior and chronic diseases, the general linear model (ANCOVA) was used to compare the subjects in terms of their menopausal symptoms.
To determine the predictors of the QOL in urban and rural women, those of the independent variables that had a P-value less than 0.2 in the bivariate tests (such as the independent t-test and Pearson's correlation test) were entered into the multivariate linear regression model in the backward strategy.
Results
This study examined 544 urban and rural postmenopausal women between March and September 2015, selected through cluster sampling. The women had a mean age of 51.8 ± 3.1 and the mean number of their children was 3.7 ± 1.3. A total of 78.9% of the subjects were housewife, 66.6% were illiterate or had primary school education and 76.6% had a moderate income. Table 1 presents the socio-demographic characteristics of the study subjects by place of residence.
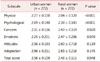
After adjusting the basic variables, the mean scores of menopausal symptoms and their subscales were compared between the urban and the rural women; the results showed significantly higher scores in the physical and psychological subscales in the urban women, while the rural women had significantly higher scores in the concern subscale. The total score of menopausal symptoms was also significantly higher in the urban than the rural women (Table 2).
According to the bivariate tests, the P-value was less than 0.2 for the variables of the number of children, satisfaction with the spouse's and children's behavior and the level of education in the urban women and for the variables the number of children, satisfaction with the spouse's and children's behavior, occupation and chronic diseases in the rural women. These variables were thus entered into the linear regression model.
The multivariate linear regression analysis showed that, in the urban women, satisfaction with the spouse's and children's behavior and housing status were predictors of menopausal symptoms and explained 47% of the variations in QOL. In the rural women, satisfaction with the spouse's and children's behavior and the duration of menopause were predictors of menopausal symptoms and explained 34% of the variations in QOL (Table 3).
Discussion
The present study was conducted to compare the pattern of menopausal symptoms, concern and attitudes in urban and rural postmenopausal women. The rural women examined in this study had a higher mean age and a lower socioeconomic status compared to the urban women.
Joint and muscle pain were the most common physical symptom in the subjects; this finding is consistent with the results obtained by Bernis and Reher20 in urban and rural areas of Spain. A cohort study on women's health in Australia found that joint and muscle pain are highly prevalent around menopause.21
The present study found significant differences between the urban and rural women in terms of the severity of physical and psychological symptoms of menopause. After adjusting the confounding variables, the urban women were found to experience the physical and psychological symptoms more commonly. The urban women experienced more hot flushes and night sweats compared to the rural women. In terms of sexual symptoms, the urban women reported lower sexual desires compared to the other group; however, no significant differences were observed between the two groups in terms of vaginal dryness. According to studies conducted in India, Spain and Mexico, Bangladesh hot flushes are more prevalent in rural than in urban women;14162021 meanwhile, psychological symptoms such as mood swings and irritability are more common in urban women. In contrast to the present findings, Martinez et al.13 found the place of residence to have no significant effects on menopausal symptoms. Moreover, a study conducted by Sagdeo and Arora22 on 500 postmenopausal women found hot flushes, joint and muscle pain and physical and mental fatigue to be more common in rural women, and urinary symptoms and heart diseases more common in urban women. These differences can be explained by the differences in lifestyle, including nutrition, physical exercise and BMI. The rural population tends to have a more active lifestyle and use less processed food containing different flavorings.
The linear regression analysis revealed the predictors of the severity of the physical and psychological symptoms of menopause to be relatively similar in the urban and rural women. Housing status and satisfaction with the spouse's and children's behavior were the predictors of menopausal symptoms in the urban women, and the duration of menopause and satisfaction with the spouse's and children's behavior were the predictors of these symptoms in the rural women.
A study conducted by Dasgupta and Ray23 in rural areas of India found the spouse's knowledge about menopause and consequently the woman's satisfaction with her spouse's behavior to be a determining predictor of the severity of the sexual symptoms of menopause and hot flushes.
The difference in the severity of the psychophysical symptoms of menopause appears to be caused by the differences in living environment. The results of the present study revealed a greater severity of physical symptoms in the urban women compared to the rural women. The physical symptoms experienced by the subjects included hot flushes, decreased sexual desire, gastrointestinal symptoms, palpitations and joint and muscle pain. All of these symptoms were more severe in the urban women except for joint and muscle pain. The urban women also experienced more severe psychological symptoms of menopause compared to the rural women. Given the stressful urban lifestyle, these results are not unexpected. The decreased sexual desire in the urban women can be justified by noting the close relationship between physical functioning and psychological symptoms. Moreover, the rural women were more worried about menopause in this study than the urban women. This difference can be attributed to the lower levels of education and knowledge in the rural women. Nonetheless, no significant differences were observed between the two groups in terms of attitude and adjustment.
Conclusion
The results of study show that psychophysical symptoms affected urban women more than they did rural women, in contrast, the rural women experienced more concern about menopause and its consequences. These findings can be explained by the differences in the cultural context of cities and villages, the mechanization of life in urban communities, the behavioral changes occurring in urban women, the different lifestyles, nutrition regimens and physical activities and also the different identity formation and decision-making processes in cities and villages.
This study had its own set of strengths and limitations; its limitations include failing to inquire the participants about their frequency of physical exercise and not using a nutrition and food intake questionnaire, while the large sample size used is considered a strength.


 XML Download
XML Download