

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Endocrine system being a complex homeostasis plays an important representation in promoting periodontitis (PD), which is characterized by inflammation of the supporting tissues of the teeth, including the gingiva, alveolar bone, and periodontal ligament. PD is a chronic inflammatory process that occurs in response to a predominantly gram-negative bacterial infection originating in dental plaque.1 PD leads to progressive and irreversible loss of bone and periodontal ligament attachment, as inflammation extends from the gingiva into adjacent bone and ligament. Signs and symptoms of progressing PD include red, swollen gums that may appear to have pulled away from the teeth, persistent bad breath, pus between the teeth and gums, and loose or separating teeth.2 Menopause archetypically occurs in the fifth decade of life in women.3 Menopause in women is a physiological state that gives rise to adaptive changes at both the systemic and oral level. Menopause literally means “without estrogen” and by definition, it is the time at which cyclic ovarian function, as manifested by menstruation ceases.4 The oral alterations noted at menopause are frequently related to hormonal changes although a physiological aging of the oral tissues also plays a contributing role.5 Gingival epithelium becomes thinner and more prone to inflammatory changes during menopause.6 On the other hand salivary flow rate and composition may be altered and contribute to the development of several oral conditions.7 Sudden decreases in estrogen production during menopause stage contemplate to be the main cause of primary osteoporosis, which also affects jawbones.8 It has been suggested that this reduction in bone mineral density could contribute to periodontal disease progression.9 In conjunction with effect on bone, estrogens also interfere with other periodontal tissues (gingiva and periodontal ligament) and influence host immune-inflammatory responses.10 In this study among pre- and postmenopause, which one is reciprocating to periodontal treatment was scrutinized.
Materials and Methods
1. Study population
This interventional pre-post clinical trial was carried out in the outpatient department of Periodontology. Study sample consisted of 60 female subjects aged between 40 and 60 years. All 60 patients meeting the selection criteria were consecutively enrolled from January 2015 to August 2015. All of them were explained about study design and obtained the informed consent before the procedure was carried out. This study was approved by local ethical committee (No. 006) and also registered under clinical trial. All clinical parameters were done by one physician. Depending on the menstrual history the patients are prorated into two groups with each group comprising of 30 individuals. Inclusion and exclusion criteria are same for both groups (Chart 1).
Group I. Thirty premenopausal women with chronic PD
Group II. Thirty postmenopausal women with chronic PD
3. Exclusion criteria
· Below 40 years of age
· With gross oral pathology or tumors
· Patients on long term steroid medication
· Undergoing hormone replacement therapy
· Pregnant women or planning for pregnancy
· Those who have received periodontal therapy in the preceding 6 months
· Those that are under medication in the preceding 6 months
· Any systemic disorders or any medication that affects the periodontal status was excluded from this study.
4. Statistical analysis
Statistical analysis was done by using IBM SPSS version 21 software (SPSS Inc., Chicago, IL, USA). Intergroup comparison and percentage decrement was done by using independent sample t-test and intra group comparison was done by paired t-test. All P-values of less than 0.05 were considered to indicate statistical significance.
Results
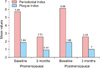
There was statistically significant reduction in the mean values of all the parameters from baseline to 3 months within the group I. The mean PRI levels have reduced from 5.68 ± 0.64 at baseline to 2.53 ± 0.13 at 3 months after treatment. The mean PI levels have reduced from 1.84 ± 0.17 at baseline to 0.91 ± 0.13 at 3 months after treatment. There is statistical significant difference between baseline and 3 months post treatment for all the parameters (P < 0.001) (Table 1).
There was also a statistically significant reduction in the mean values of all the parameters from baseline to 3 months within group II. The mean PRI levels have reduced from 6.08 ± 0.46 at baseline to 2.55 ± 0.12 at 3 months after treatment. The mean PI levels have reduced from 1.86 ± 0.24 at baseline to 1.00 ± 0.24 at 3 months after treatment. There is statistical significant difference between baseline and 3 months post treatment for all the parameters (P < 0.001) (Table 2).
Discussion
Periodontal disease is initiated by microbial pathogens that elicit a host immune response with subsequent tissue destruction of the periodontal structures, including breakdown of alveolar bone.2 Although bacteria are a necessary factor in the equation, the reaction of the host's immunoinflammatory system is responsible for most of the destruction found in periodontal disease. Thus, it makes sense that a number of environmental and acquired factors may modify a patient's risk of developing periodontal disease. Menopause triggers a wide range of changes in women's body, and the oral cavity is also not an exceptional.13 Estrogen deficiency, which affects systemically the sequence of bone resorption and formation, has received an increasing attention in relation to the stability of alveolar bone structure in postmenopausal women.14 Found wanting of estrogen in menopause, the anti-inflammatory effect of this hormone on the periodontium and its supporting structures get compromised. Another sex hormone which also plays an important role in bone metabolism during pre- and postmenopause is progesterone.
Repercussion of estrogen and progesterone function is different on different organ systems. Estrogen can influence the cytodifferentiation of stratified squamous epithelium, synthesis and maintenance of fibrous collagen. Additionally, estrogen receptors in osteoblast-like cells and receptors in periosteal fibroblasts provide a mechanism for direct action on bone as well as periodontal tissues.15 Together affect the micro circulatory system by producing the following changes: swelling of endothelial cells and periocytes of the venules, adherence of granulocytes and platelets to vessel walls, formation of micro thrombi, disruption of the perivascular mast cells, increased vascular permeability and vascular proliferation.4
Steroid hormones have been shown to directly and indirectly exert influence on cellular proliferation, differentiation and growth in target tissues, including keratinocytes and fibroblasts in the gingiva.16 Two theories were explained about the actions of hormones on the cells: 1) change of the effectiveness of the epithelial barrier to bacterial insult; and 2) effect on collagen maintenance and repair.17 Not even this, these hormones have also been shown to increase the rate of folate metabolism in oral mucosa. Since folate is stand in need of tissue maintenance. Marked up metabolism can relinquish folate stockpiles and hold down tissue repair.18 Estrogen is responsible for alterations in blood vessels of target tissues in females.19 In contrast; progesterone has been shown to have little effect on the vasculature of systemic target tissues.20 On the other hand, in gingiva and other non-periodontal intraoral tissues, more evidence has accumulated for progesterone affecting the local vasculature than for estrogen. In addition, progesterone has been shown to reduce corpuscular flow rate, allowing for accumulation of inflammatory cells, increased vascular permeability and proliferation.21
Menopause and the lack of ovarian steroids are known to promote important changes in connective tissue. The mechanisms involved in this influence are not completely understood, but it is thought to be related to the action of estradiol on the connective tissue.22
During the menopause estrogen deficiency is one of the most frequent causes of osteoporosis in women and a possible cause of bone loss and insufficient skeletal development in men. During bone growth estrogen is needed for proper closure of epiphyseal growth plates both in females and in males. Estrogen deficiency leads to increased osteoclast formation and enhanced bone resorption. In menopause estrogen deficiency induces cancellous as well as cortical bone loss.23 These hormones may alter immunologic factors and responses, including antigen expression and presentation, and cytokine production, as well as the expression of apoptotic factors, and cell death.24 Several studies have focused on the observation that immune system components have been identified as possessing sex steroid receptors.16 Progesterone in particular has been shown to stimulate the production of the inflammatory mediator, prostaglandin E2 and to enhance the accumulation of polymorphonuclear leukocytes in the gingival sulcus.25 In addition, sex steroid hormones seem to modulate the production of cytokines,26 and progesterone has been shown to down regulate interleukin-6 (IL-6) production by human gingival fibroblasts to 50% of that of control values.27
The steroid metabolites may also contribute to nutritional requirements of the pathogens, or enable synthesis of matrices associated with host evasion mechanisms.28 Culture supernatants of these micro-organisms have been shown to enhance the expression of 5α-reductase activity in human gingiva and in cultured gingival fibroblasts, resulting in the formation of 5α-dihydrotestosterone (DHT) from androgen substrate.29 The DHT can influence protein synthetic activity in these pathogens, for which there is a variety of applications. Some of these functions are: 1) the formation of surface capsular protein contributing to their evasion of host elimination mechanisms, such as phagocytosis, by preventing opsonisation; 2) persistence and dissemination with the host; and 3) interspecies aggregation and energy generation as a result of the electron transfers involved in these enzyme activities.28 Five-α-reductase activity can be activated in a phospholipidic environment. Increased amounts of phospholipases A2 and C are synthesized by periodontal pathogens (e.g., spirochaetes) during inflammatory episodes in the periodontium. Phospholipase C is also released from leukocytes during cell lysis and in addition to degrading gingival crevicular epithelium it is also known to stimulate 5α-reductase activity.29
Several studies have concluded that the relation between the risk of postmenopausal tooth loss and estrogen replacement. Decrease in estrogen levels have been linked to inflammation of gingiva and reduced levels of clinical attachment.30 Many authors demonstrated a potential correlation between ovarian dysfunction and an increased incidence of periodontal disease.31 There is no published data regarding evaluation of periodontal status in pre- and postmenopausal women with PD following non-surgical therapy. Till date no such study was done, as per my knowledge this is the first study comparing pre- and postmenopausal women periodontal status. Since both pre- and postmenopausal conditions are disproportion of hormones and due to imbalance of host inflammatory as well as other functional cells, both conditions are thought-out as inflammatory conditions leads to destruction of other body parts including oral cavity.3233 But only these hormones itself are neither responsible nor sufficient to produce changes in gingiva by themselves. However, they may alter responses of periodontal tissue to microbial plaque and thus indirectly responsible for severity of periodontal disease.3 In this study both groups reciprocated consequence results for non-surgical periodontal treatment. This shows proper oral hygiene maintenance and plaque control might counteract disastrous effects which are caused by hormonal dysfunction. Treatment of periodontal disease has been primarily directed towards a microbiological etiology.253435363738 Prevention of bone loss by modulating the host response to infection could be a new adjunctive method for the management of PD.3940 Apart from maintenance of a meticulous oral hygiene, several studies have indicated that estrogen therapy builds up mandibular bone mass and diminishes the severity of periodontal disease in postmenopausal women.3141
First, limitation was short sample size of this study. Second, longitudinal studies conducted on larger sample size might provide precise results. Third, identification of inflammatory markers would have been more specific.
Conclusion
This study emphasizes on the effects of pre- and postmenopause on periodontal disease progression. It is also clear that not all patients and their periodontium respond in the same way to similar amounts of circulating sexual hormones. There was better response to non-surgical periodontal therapy in premenopausal women when compared to that of postmenopausal women with chronic PD suggesting that even severe inflammatory conditions which are exaggerated by other influencing factors become less intense with non-surgical periodontal therapy. With these results we can put forward that the influence of sex hormones can be minimized with good plaque control. Prevention and early management of oral disorders is priority in women's health research. Physicians caring for postmenopausal women should be wakeful and embolden their patients to seek regular dental checkups.




 XML Download
XML Download