

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Obesity is now recognized as a major public health problem that constitutes a risk factor for life-threatening diseases such as type 2 diabetes and cardiovascular disease (CVD), as well as some types of cancer.1 These disorders represent major causes of morbidity and mortality in industrialized countries and are increasing problems in developing countries as well.2
Obesity as the most common disorders in climacteric women occurs in approximately 65% of them3 due to alterations in visceral adipose tissue metabolism.45 Menopause is associated with a rise in follicle-stimulating hormone and luteinizing hormone levels and a fall in estrogen.6789 Women have more body fat compared to men, and there is a gender-specific difference in fat distribution. In women, adipose tissue is accumulated especially around the hips, buttocks, and thighs while men have a larger intra-abdominal fat mass.1011 Pedersen et al.12 demonstrated that estradiol, binding to its receptor α, inhibits adrenaline-stimulated lipolysis in human subcutaneous fat cells by increasing the amount of α2-adrenergic anti-lipolytic receptors. This may explain how estradiol is related to typical female subcutaneous adipose tissue distribution because this inhibition is not observed in visceral fat depots. In women, estradiol may shift accumulation of fat from visceral into subcutaneous depots.12 Redistribution of body fat, after menopause, is associated with CVD1011 and metabolic syndrome as well.13
In a recent study, ovariectomy (OVX) in rats resulted in a progressive accumulation of fat in the abdomen, increased risks of insulin resistance, dyslipidemia and CVDs.1415 Adipokines are an exciting new link between obesity, insulin resistance and CVD.1516 Apelin is a recently identified bioactive adipokine. It is an endogenous of the orphan seven-transmembrane (TM) domain G protein-coupled receptor, putative receptor protein related to the angiotensin receptor AT1 (APJ), which is functionally similar to angiotensin-1 coupled receptor.1718
Existence of apelin and its receptor in various tissues of human and mice such as: hypothalamus, anterior pituitary, endothelial vessels, heart, lungs, stomach, kidney, mammary glands, thyroid, ovarian, colon mucus, pancreas, adipose tissue, liver and muscle reveal the widespread role of this hormone.181920212223242526272829 The hormone regulates adipose tissue's growth and has a role in the process of chronic inflammation caused by increased adipose tissue and stress.2428 Apelin upregulates sex steroids, insulin, tumor necrosis factor-α and growth hormone in adipose tissues of human and mice.1923242526272829 This cytokine is involved in regulation of fluids and food intake in the hypothalamus22 and increases in apelin concentration results in energy consumption.303132
Regarding the fact that visceral fat is the source of adipokines, more notably, apelin, we hypothesized that estrogen deficiency might be one possibility for apelin level reduction and consequently visceral fat accumulation with other clusters of metabolic syndrome components.
To our knowledge relationship between plasma apelin concentration and estrogen treatment has not been studied yet. Therefore, the purpose of this study was to determine the effect of estrogen replacement therapy on visceral fat, serum apelin level. To approach these goals, we used OVX rats as a model of menopause.3334353637
Materials and Methods
Female Wistar rats (n = 30), weighing 180 to 200 g (2 months of age) were used in this study. Except for sham group, all animal underwent OVX surgery according to the technique described by Babaei et al..33 For surgery, rats were anesthetized using a mixture of ketamine- xylazine (61.5-7.6 mg/kg, i.p.). Animals were housed four per cage and fed standard pellet rat chow and had free access to tap water. The 12:12-hour light: dark cycle started at 07:00 hour and the room temperature was kept at 21 to 23oC. The experiments described in this report were conducted according to the policy of Ethics Committee of the Guilan University of Medical Sciences.
1. Groups and treatment protocol
Thirty Female Wistar rats were divided into three following groups: OVX (n = 20) and sham (n = 10) groups. OVX rats were subdivided into estrogen replacement therapy (OVX+est; n = 10), and sesame oil therapy (OVX+ses oil; n = 10) groups. Rats in the OVX+est group received subcutaneous injections of 17β-estradiol valerate (30 mg/kg body weight; Sigma-Aldrich Corp., St. Louis, MO, USA) dissolved in 0.2 mL sesame oil (Aburaihan Pharma Co., Tehran, Iran), three days a week, for eight weeks. Rats in the OVX+ses oil group received the same volume of sesame oil. All rats were weighed twice a week, between 09:00 and 11:00 to yield a weekly weight for each animal, two weights were averaged. To measure the food intake, an equal amount of food (20 g/day/rat) was given to all rats and their consumption was measured the following day by subtracting the remaining uneaten food from the total given one. All experimental groups had initially similar mean body mass and were treated similarly in terms of daily manipulations. Body weight, food intake, and visceral fat were measured using the accurate to 0.1 g scale (Sartorius, Goettingen, Germany).
2. Analytical procedure
1) Body mass index (BMI)
All rats were weighed twice a week, between 09:00 and 11:00. A weight average was obtained for each animal. The height of the animal was measured under general anesthesia from tip of nose to the anus. BMI was measured dividing weight by the square of height (g/cm2).
2) Blood sample
The food was removed from the animal's cage at least 24 hours before scarification. After complete anesthesia, the abdominal cavity was rapidly opened and blood samples were drawn from the inferior vena cava. The serum was immediately separated by centrifugation (3,000 rpm for 15 minutes) and stored at -80℃ for later biochemical and hormonal measurements.
Serum apelin concentration was measured by rat apelin enzyme-linked immunosorbent assay kit (Shanghai Crystal day Biotech Co., Shanghai, China). The serum glucose concentration was determined by enzymatic (glucose oxidase-amino antipyrine) colorimetric method (Pars Azmoun, Tehran, Iran) and Serum total cholesterol (TC) and high-density lipoprotein cholesterol (HDL-C) were determined by enzymatic (Pars Azmoun) colorimetric method. Serum triglyceride (TG) was determined by enzymatic (Pars Azmoun) colorimetric method. Serum glucose, cholesterol, TG, HDLC, and low-density lipoproteins cholesterol I (LDL-C) were determined like our previous works.3839 After collecting the blood samples, all intra-abdominal fat depots including mesenteric, urogenital and retroperitoneal were dissected out by one experimenter and weighed immediately after dissection to avoid evaporative weight loss. Mesenteric fat pad consisted of adipose tissue surrounding the gastrointestinal tract from the gastroesophageal sphincter to the end of the rectum. Urogenital fat pad included adipose tissue surrounding the kidneys, ureters, and bladder as well as ovaries, oviducts, and uterus. The retroperitoneal fat pad was taken distinctly behind each kidney along the lumbar muscles.
3) Statistical analysis
All data are presented as mean ± standard error (SE) before statistical analysis, normal distribution and homogeneity of the variances were tested by K-S test. Statistical comparisons between groups were performed by one-way analysis of variance test, followed by Tukey's post-hoc test. Levels of statistical significance were set at P < 0.05.
Results
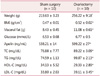
Two weeks after OVX, visceral fat (P = 0.006) and body weight (P = 0.001) of OVX group were significantly increased compared with the sham group and remained elevated even after 8 weeks of surgery (P = 0.02, P = 0.004) respectively (Table 1).
Serum glucose, TC (P = 0.004) and HDL-C (P = 0.027) and LDL-C (P = 0.022) also showed elevation after two weeks of OVX.
No significant difference was observed in visceral fat, blood lipids and plasma apelin concentration between OVX+est and OVX+ses oil groups after eight weeks of treatment. However, estrogen therapy reduced body weight compared with the OVX+ses oil group (Table 2).
Discussion
Our results showed a significant difference in body weight, height, BMI, visceral fat, weight, glucose level, blood lipid profile, and serum apelin between the OVX and sham groups, two weeks after surgery. These findings partly are in agreement with the results of our previous study40 and Al-Wahaibi and colleagues41 indicating the significant increase in body weight of OVX rats after one month.
Ten weeks follow-up in our study showed that increase in body weight and visceral fat in OVX rats remained elevated compared to the control group. This is in agreement with the findings of several studies showed an increase in visceral fat after hypoestrogenism.414243 OVX may stimulate adipocyte hypertrophy and increased levels of epidermal growth factor, therefore OVX rats will be promoting obesity.3839
The results of 8-week estrogen therapy in the present study revealed that a significant reduction in body weight and BMI. While no significant difference was observed in visceral fat, blood lipids and plasma apelin concentration between OVX+est and OVX+ses oil groups after eight weeks of treatment.
Based on the results of studies in in-vivo and in-vitro condition, estrogen receptors play a major role in the regulation and distribution of body fat and are correspondence for lipolytic effects of estrogen.44 Therefore, our results in line with other similar studies42434546 indicate an increase in body weight after OVX with increase of fat mass, especially visceral one. No significant difference in the average of food intake between OVX+est and OVX+ses oil groups confirms that estrogen induces weight loss through other mechanisms rather than central mechanisms of food intake. Although the mechanisms of estrogen on body weight has not been fully understood, but the study carried out by Ryan et al.47 showed that ovarian steroid hormones involved in the regulation of obese gene and corticosterone hormone.
According to D'Eon et al.48 estrogen therapy leads to weight reduction. In the present study, a significant reduction in body weight after estrogen therapy is not in parallel with a reduction in visceral fat. The data found in our study on visceral fat is consistent with Ryan et al.47 and Sites et al.49 in postmenopausal women after hormone replacement therap. However, some studies showing contradictory results of estrogen on visceral fat in postmenopausal women495051 and OVX rats as well.42 D'Eon et al.48 were reported a reduction in visceral adipose tissue and adipocytes size in OVX rats after estrogen therapy. They found increased rate of adipocytes lipolysis and down-regulation of related genes, such as lipoprotein lipase in abdominal adipose tissue after injection of estradiol. They also showed that in muscles, estradiol led to up-regulation of lipoprotein lipase enzyme and peroxisome proliferator-activated receptor (PPAR-γ).48 Therefore, fat oxidation and adipocytes lipolysis cause fat usage as the main source of body fuel.42 In addition, the loss of ovarian estrogen causes increasing in cell size, lipolysis speed and lipoprotein lipase activity in visceral adipose tissue.4852 The findings of this study showed insignificant changes in serum apelin after eight-week in the OVX+est compare to OVX+ses oil group. While serum TG levels in response to estrogen therapy were increased insignificantly. This finding is consistent with results of the study showed that hormone therapy has a negative impact on TG levels.51 This finding is in contradictory with the results of those studies reported that hormone therapy has a positive effect on the cardiovascular system.5153 However, there is little information for explaining the results of the effects of estrogen therapy on the relationship between apelin and visceral fat level. Cross-sectional and short-term replacement of estradiol, the method for measuring visceral fat can likelihood affect the relationship between the two variables. Studies have shown that hypoestrogenism coincides with hyperlipidemia, hyperinsulinemia, and hypertension, the most important components of metabolic syndrome.54 On the other hand, increasing in cytokines such as apelin is associated with hypertension, heart failure, obesity,5556 hyperglycemia and atherogenic effects5758 and also according to studies Apelin can be used as a specific marker for insulin sensitivity and lipid profile and this adipokine might play a role in the pathogenesis of polycystic ovarian syndrome.596061626364 No significant change in serum apelin of OVX rats after estrogen replacement indicates that serum apelin concentration was found to be regulated by other factors such as nutrition, growth hormone, cortisol,29 and also liver function65 rather than estrogen per se. Future studies with long-term intervention are suggested to clarify the relationship between the cytokine apelin and estrogen considering molecular signaling.

 XML Download
XML Download