

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Menopause marks the limits of the period of women's fertility.1 In fact, menopause is a normal event in women's life and everywoman will experience it throughout her life.2 During the last century, due to promotion of public health and application of modern methods in treatment, life expectancy has almost doubled in the developing countries.3 The Iranian population of postmenopausal women is assumed to be approximately 3.5 million.4 About 30 years of women's lives are spent in the menopause or postmenopausal period.5 Preventing and postponing of women's disabilities and maintaining their health is the most important issue of public health at the present time and in future. Menopause is a kind of developmental stage and critical period that entails many complications which can have impact on the lives of women and undermine their sense of well-being.6 During menopause, production of estrogen is stopped in ovarian and vasomotor symptoms are declined. In addition, women experience symptoms like hot flashes, night sweats, atrophy in vaginal and vulva, and some other complications that affect their quality of life.5 Menopause in most cultures is equal to aging in women. Many women in menopause period feel a loss, such as loss of motherhood, youth, beauty, and life.7 However, some women experience positive emotions at this time, for example it has been shown that postmenopausal women have a better feeling of power and freedom. Since there is no fear of pregnancy, they experience sexual relationship with more pleasure. Relief from menstrual and premenstrual syndrome was one of the positive aspects cited by these women.8
Marital satisfaction is the positive and enjoyable attitude that a couple experience from different aspects of their sexual relationships. Marital satisfaction is an identical feeling of happiness, satisfaction, and joy experienced by women or men when covers all common aspects of their lives. Health and well-being of a family depends on healthy and thriving relations of couples and if the family foundation does not have the necessary strength, its negative consequences will cause a variety of physical and mental problems. Satisfying relationships bring many benefits for couples. One of these benefits includes increasing mental and physical health of women, their husbands and children, as well as improving their flexibility in the pressures of life.9 One of the concerns in menopausal period is the loss of sexual desire or sexual satisfaction. Sex satisfaction is an important factor in marital satisfaction.10 The decrease of sexual attraction, sexual desire, and sexual activity are the most common complaints in postmenopausal women, which may be caused by the reduction of estrogen and androgen hormones in post-menopause period.11 Husband is the most important and closest person who can support his menopausal women through this developmental crisis by proper understanding of the situation and the related problems. Despite the fact that having the necessary knowledge and awareness about menopause is necessary for social support, unfortunately husbands' information about menopause is very low.12 According to the different cultural contexts in different areas, such research must be carried out in different areas. Also, most studies have been conducted on training postmenopausal women while training their husbands was rarely investigated. Hence, the present study targeted to investigate the effect of health education of postmenopausal women's husbands on the women's marital satisfaction.
Materials and Methods
1. Participants and setting
The present study was a randomized controlled trial with two parallel arms in which participants were selected with a ratio of one to one. The study protocol was approved by the Research Council of Shahid Sadoughi University of Medical Sciences and Health Services, Yazd, Iran (registration code: 92/11). It was also registered on ClinicalTrials.gov with the registration ID of NCT01652300.
A total number of 100 participants were randomly selected and then classified in two equal groups (n = 50). The study was conducted from May to August 2014 in Yazd, Iran. More detail of study protocol is explained elsewhere.13
2. Intervention program
The eligibility of the randomly selected participants was evaluated through phone calls. The eligible individuals were invited to participate in the study. All participants in the intervention group were requested to attend a briefing session with their spouses. At the beginning of the session, written informed consent was obtained from all participants and their spouses. The participants were then asked to complete the demographic questionnaire and the Evaluation and Nurturing Relationship Issues, Communication and Happiness (ENRICH) questionnaire. The spouses also filled out the demographic questionnaire and the questionnaires on their knowledge and performance about menopausal health. Afterward, the spouses attended the first training session. The educational content, including symptoms and complications of menopause and management options, as well as the role of spouse support during transitional period, was extracted from reference books and guidelines for health care during menopause provided by the Ministry of Health and Medical Education of Iran.14 The educational program was comprised of three 60-minute sessions, in which a combination of different educational methods (e.g., lectures and questions and answers) and educational aids (e.g., video projectors and video players) were used. The educational sessions were held by the third author who was skilled in the field of menopause. At the end of the program, the participants were provided with training pamphlets and the researcher's telephone number (in case they had a question). The control group did not receive any intervention. These participants and their spouses were invited individually to complete the questionnaires in the presence of the researcher. They were also asked not to seek information on menopause health during the study period.
Three months after the intervention, the ENRICH questionnaire and the questionnaires on the men's knowledge and practice about menopause were completed again. To observe research ethics, the control group was provided with training pamphlets containing the content of the educational sessions at the end of the study.
3. Study instruments
In addition to the mentioned questionnaires, ENRICH's 47-item (1990) questionnaire was applied to determine the participants' level of marital satisfaction. The original form of this inventory consisted of 115 questions and 12 scales which was used by Olson to assess marital satisfaction. He believed that each item in this inventory is related to one of the most important areas of marital satisfaction. While validity of marital satisfaction inventory was approved in several studies, the reliability of ENRICH marital satisfaction inventory was calculated as 0.95 in the present study. Using Cronbach's alpha (α) coefficient, Elson, Forinero, and Drakman (1998, according to Eqbal, 2010) reported the reliability of the questionnaire to be 0.92.15
Soleimanian16 calculated the test's correlation for the first time in Iran and reported the long and short form correlations equal to 0.93 and 0.95, respectively. Further, the α coefficient for Soleimanian's questionnaire was equal to 0.95.15 This questionnaire consists of 47 items all of which have to be answered on a 5-point Likert scale. One part of items deals with satisfaction and is scored from 5 to 1, (i.e., 5 = totally agree, 4 = agree, 3 = not agree not disagree, 2 = disagree, and 1 = totally disagree), the other part's scores indicate dissatisfaction and disagreement and range from 1 to 5 (i.e., totally agree = 1, agree = 2, neither agree nor disagree = 3, disagree = 4, totally disagree = 5). Scores can range from 47 to 235, with higher scores indicating greater marital satisfaction.
Marital satisfaction was investigated in the six following categories: very unsatisfied, unsatisfied, satisfied, relatively satisfied, very satisfied, and extremely satisfied.
4. The 9 scales of ENRICH inventory (47 items) include
1) Personality issues
This scale examines an individual's perception of his or her partner with regard to behavioral issues and the level of satisfaction felt on those issues.
2) Communication
This scale is concerned with an individual's feelings and attitudes toward communication in his or her relationship. Items focus on the level of comfort felt by the partner in sharing and receiving emotional and cognitive information.
3) Conflict resolution
This scale assesses the partner's perception of the existence and resolution of conflict in the relationship. Items focus on the openness of partners to recognize and resolve issues and the strategies used to end arguments.
4) Financial management
This scale focuses on attitudes and concerns about the way economic issues are managed within the relationship. Items assess spending patterns and the care with which financial decisions are made.
5) Leisure activities
This scale assesses activities in spending free time. Items reflect social versus personal activities, shared versus individual preferences, and expectations about spending leisure time as a couple.
6) Sexual relationship
This scale examines the partner's feelings about the affectional and sexual relationship. Items reflect attitudes about sexual issues, sexual behavior, birth control, and sexual fidelity.
7) Children and parenting
This scale assesses attitudes and feelings about having and raising children. Items focus on decisions regarding children's discipline and goals, as well as the impact of children on the couple's relationship.
8) Family and friends
This scale assesses feelings and concerns about relationships with relatives, in-laws, and friends. Items reflect expectations for and comfort in spending time with family and friends.
9) Religious orientation
This scale examines the meaning of religious beliefs and practices between the couple. Higher scores indicate more importance of religion in the marriage (5 items).
Table 1 below represents this ENRICH inventory questionnaire's descriptive information.
5. Statistical analysis
Continuous data were reported as mean ± standard deviation (SD). The normality of data distributions was tested using the one-sample Kolmogorov-Smirnov test. Independent t-tests were performed to compare continuous variables with normal distribution. Follow-up analyses included an independent t-test at each time point. The level of significance was set at P value less than 0.05. All analyses were carried out using SPSS software (SPSS Inc., Chicago, IL, USA).
Results
Although 109 women were initially selected, 9 were excluded and 100 women (50 in each group) completed the study (Fig. 1).13
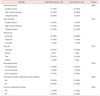
The average age of men in the intervention and control groups were 52.1 ± 3.3 and 52.2 ± 3.0 years, respectively, while those of women in the intervention and control groups were 49.8 ± 2.7 and 50.1 ± 2.5 years, respectively. Further, the average ages of marriage for men in the intervention and control groups were respectively 24.66 ± 3.44 and 25.1 ± 3.3 years. The average number of children in the intervention group was 2.9 ± 1.2 while it was 2.8 ± 1.2 for the control group which according to the independent t-test no significant difference was observed in these variables between the two groups (P>0.05) thus it can be said that the two groups matched (Table 2). In terms of education, 18% of men and 22% of women had elementary and secondary education, 57% of men and 57% of women had high school and diploma education, and 25% of men and 21% of women had academic degrees. 29% of men had government jobs, 57% were self-employed, and 8% were retired. Twenty-three percent of women were employed while 77% were housewives. According to Chi-square test, no significant difference was observed between the two groups in terms of education and occupation (P>0.05) (Table 3).
The average age of menopause in the intervention group was 48.26 ± 1.34 and in the control group 48.32 ± 1.43 years, also, the average age of menarche in the intervention and control groups were 11.84 ± 1.31 and 11.73 ± 1.4 years, in order. Based on the independent t-test there was no significant difference between the two groups (P>0.05) (Table 2).
Before the intervention, the mean scores of knowledge and performance of men in the intervention and control groups as well as marital satisfaction scores among women in these two groups showed no significant difference (P>0.05).
The paired sample t-test results indicated a significant difference between the men's knowledge scores about menopause before and after the educational program in the intervention group (P=0.001). But in control group the average score of knowledge before the education program and two months after it had no significant difference (P=0.729). Also, the average score of men's performance about menopause in the intervention group had significant difference before the education and two months after it (P=0.001), while in the control group no significant difference was observed (P=0.394).
Although the two groups had no statistically significant differences in terms of baseline scores of their knowledge and performance (P>0.05), post intervention knowledge scores were significantly higher in the intervention group than in the control group (P<0.0001). Student's t-test results also indicated a significant improvement in husbands' performance about menopause in the intervention group two months after the educational program (P<0.0001). Moreover, in the intervention group, paired t-test suggested significant differences in the spouses' knowledge and performance scores before and two months after the intervention (P<0.0001). No such significant differences were detected in the control group (Table 4).
The results of paired t-test showed that there was no significant difference in control group before and after the intervention, but the total average score of marital satisfaction and its nine sub-scales, except in personality scale, was significantly higher in the intervention group than the control group (P<0.05). This is while there was no significant difference in the control group (P>0.05) (Table 5).
The results of independent t-test showed that there was no significant difference in women's total average score of marital satisfaction and its nine sub scales between the intervention and control groups before the intervention (P>0.05). But after the intervention there was a significantly higher score for the intervention group, except for the personality, financial management, sexual orientation, and religious orientation scales (P<0.05).
Discussion
This study indicated a significant difference in total satisfaction scores and scales of marital communication, conflict resolution, leisure activities, marriage and children, as well as relatives and friends between postmenopausal women of the intervention group, whose husbands were trained about menopause, than the members of the control group whose husbands received no trainings. But no significant difference was observed in the scales of personality, financial management, and sexual and religious orientations. This findings were in the same line with those reported by Clements et al.17, Fincham et al.18, and Hahlweg and Richter.19 In order to clarify these findings, Hawkins et al.20, showed that the training empowerment programs, teach couples the required skills to face the challenges of married life and prepare them to cope with marital problems efficiently. One of the very important aspects of a marital system is the amount of satisfaction that married couples experience. Thus, policy makers in many countries are trying to design and implement programs to help couples who are experiencing marital problems and conflicts. They are helping couples to face and achieve a successful and reliable marital life. One of the most important parts of this new policy in the field of family is to design and support educational programs to empower couples.21
Findings of the current study supports Olleya et al.,22 results reporting that educational empowerment does not have any significant effect on religious orientation component, however, these findings are not consistent with those reported by Ahmadi and Hossein-abadi23. To justify these findings, it seems safe to say that the educational program implemented for men to improve their marital satisfaction was not sufficient on the religious orientation. Arieta24 introduced training, raising awareness, and couples' control as the causes of gaining interpersonal skills and marital satisfaction.
Lack of educational and communicational skills is related to many of couples' problems. If couples be aware of each other's needs and wishes in different ages and then be able to satisfy these needs properly, they will certainly increase their marital satisfaction. Trying to increase menopause health awareness among men, can increase their wives' confidence and help menopausal women to have a positive attitude towards it. It also increases their marital satisfaction and improves their life quality during menopause and after it.
Conclusion
The results of this study showed that implementation of training programs and increasing men awareness on menopause health, can increase their wives' marital satisfaction. Since the educational programs conducted for men in this study were cross-sectional and short-term, one of the limitations of this study was the fact that medium-term and long term results were not assessed which should be examined in studies with larger samples and a longer time. Hence husband is the closest person who can support his menopausal wife in this critical development by understanding her problems, it is recommended to start educational programs about menopause health several years before its occurrence for couples who are in transition towards menopause and aging and continue them continuously.




 XML Download
XML Download