

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Carpal tunnel syndrome (CTS), a median nerve compressive lesion at the wrist, is the most common entrapment neuropathy and a common disorder in women.12 Although there is a long list of causes leading to increased pressure on the median nerve at the wrist, idiopathic CTS outnumbers all other types. It often occurs in middle-aged women without other known pathologies. Because of the higher CTS incidence in women particularly around menopause, the role of specific risk factors for females and hormonal changes related to menopause has been proposed.2 In a study by Kim et al.3, increased expressions of estrogen receptor alpha and beta (ERα and ERβ) in the tenosynovial tissues of postmenopausal women with CTS was found.3 Although Toesca et al.4 found expression of ERα in both transverse carpal ligaments (TCL) and synovial tissues and progesterone receptor (PR) in TCL samples from CTS patients, no statistically significant difference between male and female groups in the number of ER- and PR-positive cells within TCL or synovial tissue of CTS patients was seen with the exception of the 50 to 70 year age group. Despite these findings, the effect of sex hormones on CTS independent of other risk factors which may be different among men and women such as hand and wrist anthropometrics (higher wrist ratio, higher shape index, and narrower outlet in women) is not clear.567
Electrodiagnosis is the gold standard test for CTS diagnosis and an appropriate tool for its severity determination. Boston questionnaire is a valid and reliable tool for assessment of functional status and clinical severity in patients with CTS.89 In this study, we aimed to consider whether ER expression in TCL and serum estrogen level as two sex hormone related factors are different between post-menopausal women with idiopathic CTS who had undergone carpal tunnel release and those operated due to hand pathologies other than CTS. Also, to investigate whether sex hormones have any effect on clinical or electrophysiological severity of CTS, the relationship between these factors and either electrodiagnostic parameters or functional status according to the Boston score in the group of women with CTS was assessed.
Materials and Methods
We selected and enrolled case and control subjects from those 50 to 70 year old women admitted for hand surgery if they had severe CTS and experienced menopause for at least one year.
Patients with a history of systemic diseases such as obesity (body mass index [BMI] ≥ 30 kg/m2), diabetes mellitus, thyroid dysfunction, malignancy, rheumatoid disorders, renal dysfunction, neurological disease, previous hand fracture, hand tumor, diagnosis of peripheral neuropathy or other neuropathies based on nerve conduction studies, those who received prior hormone therapy, chemotherapy or radiotherapy, and patients with a history of alcohol consumption were excluded from both case and control groups. These conditions were diagnosed by reviewing medical history and physical examination of subjects and performing laboratory investigations, including complete blood count, erythrocyte sedimentation rate, C-reactive protein, rheumatoid factor, fasting blood sugar (FBS), thyroid function tests, blood urea nitrogen (BUN), and creatinine. Finally, 12 postmenopausal women with idiopathic CTS who decided to undergo surgery as the case group and 10 postmenopausal women without findings of CTS admitted for surgery due to other hand pathologies (except hand tumor) as the control group were recruited. The study protocol was approved by our university Ethics Committee and written informed consents were taken from subjects before taking part in the survey.
To confirm a diagnosis of severe CTS and rule out other neuropathies, we performed a conventional electrodiagnostic test by a Medelec synergy electromyography (EMG) instrument (VIASYS Healthcare UK, Surrey, UK) at a room with constant temperature of 22℃ to 24℃. The skin temperature during all the tests was 32℃. In mid-palm antidromic test, active (E1) electrode (ring, clip or bar electrode) was placed on the midpoint of the 3rd digits and the reference (E2) electrode was attached 4 cm distal to the E1 electrode. Stimulating cathode with anode proximal was placed 7 and 14 cm proximal to E1 at the mid-palm and wrist between tendons of the flexor carpi radialis and palmaris longus, respectively. A band pass of 20 Hz to 2 kHz, a sweep speed of 2 ms/div and a sensitivity of 20 µV/div were used. For motor median nerve conduction study, the E1 electrode was placed on the most prominent eminence of the thenar area halfway between the midpoint of the wrist crease and the midpoint of the first metacarpophalangeal joint in the volar aspect. The E2 electrode was attached on the proximal phalanx of the thumb. Wrist stimulation was applied 8 cm proximal to the E1 at the wrist, between the tendons of the flexor carpi radialis and palmaris longus. A band pass of 8 Hz to 8 kHz, a sweep speed of 10 ms/div and a sensitivity of 2 mv/div were used.8 Needle EMG was done for abductor pollicis longus muscle. Severe CTS was considered for patients with any evidence of axon loss including absent or low amplitude sensory nerve action potential, low amplitude or absent compound motor action potential or a needle EMG with fibrillation potentials or motor unit potential changes.10
Demographic data including age, level of education and occupation as well as BMI, duration of menopause, age at menopause, and number of parity of both cases and controls were recorded. A Persian version of Boston questionnaire the validity and reliability of which have been established by Rezazadeh et al.11, was used for the assessment of severity and functional status in patients with CTS.
Case and control specimens of the TCL were collected from all patients operated for CTS or other hand pathologies. After removing tissue samples, all specimens were fixed in 10% formalin and routine histologic paraffin sections were made and stained with hematoxylin and eosin. Sections were cut to 3 and 4 µm thickness and mounted on poly-L-lysine-coated slides. The sections were deparaffinized in xylene and rehydrated in alcohol. Then, they were heated in a microwave oven for 10 minutes in 0.01 M sodium citrate buffer (pH 6.0).
Endogenous peroxidase was blocked with 3% hydrogen peroxide/methanol. The sections were incubated overnight with a mouse monoclonal antibody against ER antigen (Clone 1 D 5; ready to use, Dako, Glostrup, Denmark) as primary antibody. After that, the slides were rinsed gently with phosphate-buffered saline and an Envision dual link system-horseradish peroxidase (HRP; ready to use, Dako) was used as the secondary antibody. Incubation with 3,3'-diaminobenzidine tetrahydrochloride was performed for 10 minutes as a substrate chromogen solution to produce a brown color. Finally, the sections were counterstained with Mayer's hematoxylin. Appropriate positive and negative control sections were processed in parallel. For immunohistochemical evaluation, the sections were evaluated under a light microscope and mean staining intensity of the fibroblast nuclei in 10 microscopic fields (original magnification, ×400) was classified semiquantitatively compared to the positive control section. The cells with complete nuclear staining were considered 3+ positive. ER immunoreactivity was measured by two independent observers. For serum estradiol determination, blood samples were collected and centrifuged at 4400 rpm for 5 minutes. The sera were isolated. Serum estradiol level was determined using estradiol enzyme-linked immunosorbent assay (ELISA) kit (IB78239; Immuno-Biological Laboratories, Minneapolis, MN, USA). Normal range of estradiol for postmenopausal women was considered < 13 pg /mL.
Data were analyzed using the SPSS for Windows version 22 software (SPSS Inc., Chicago, IL, USA). Data were reported as mean ± standard deviation (SD). Chi-square test and independent samples t-test were used to compare the group differences for qualitative and quantitative variables, respectively. Also, Spearman and Pearson correlation coefficient tests were used for assessing the correlation between variables. In all statistical analysis, P < 0.05 was considered significant.
Results
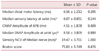
The mean ages of the case and control groups were 58.3 ± 5.6 and 60.3 ± 6.3 years, respectively (P = 0.477). The age range was 50 to 65 years in the case and 52 to 69 years in the control group. There was no statistically significant difference in demographic data and BMI between cases and controls (Table 1). The mean Boston score was 75.83 ± 5.749 with the range of 63 to 84 in the case group. No women had surgical menopause and no one had been treated with hormone replacement therapy (HRT).
No significant difference in duration of menopause (8.58 ± 7.47 and 10.20 ± 6.14 in case and control groups respectively, P = 0.591), number of parity (6 ± 2.37 and 6.2 ± 3.52 in case and control groups respectively, P = 0.876) and age at menopause (50.41 ± 5.03 and 50.30 ± 1.56 in case and control groups, respectively, P = 0.945) was observed between the groups.
Serum estrogen level was not significantly different between cases and controls (0.29 ± 0.66 and 0.34 ± 0.75 in case and control groups, respectively, P = 0.875). Also, no statistically significant difference in ER expression between case and control groups was found (Table 2).
Five patients in the case group had no recordable sensory nerve action potential. Thus, for analysis of the correlation between sensory latency, amplitude and conduction velocity and Boston score, the data of seven patients were used. There was a significant correlation between neither ER expression nor serum estrogen level and electrodiagnostic parameters and Boston score (Table 3, 4).
Discussion
We could not find any significant difference in ER expression, serum estrogen level, duration of menopause, age at menopause and parity between the case and control groups. The association between parity and CTS is controversial. In a study by Kaplan et al.12, the mean parity was significantly higher in postmenopausal women with CTS while Ferry et al.13 found a weak, but statistically significant, overall link between parity and CTS. In contrast to these studies and in the same line with our results, Dieck and Kelsey14 demonstrated that the parity was not associated with an increased or decreased frequency of the CTS. The two latter studies were not just on post-menopausal women. Dieck and Kelsey14 included 40 women in 45 to 74 year age range with CTS regardless of pre- or post-menopausal status. It brings to mind that the role of parity becomes evident after menopause; however, we could not find such a result. The small sample of our study as well as differences of culture and socioeconomic level between the case and control groups and contributing factors in child rearing may be the reason of inconsistencies in the results of studies on the parity. For example, Ferry et al.13 found an overall trend of increasing CTS risk with lower social class. Also, according to the studies with positive association between parity and CTS, it is not clear that this relationship is the result of hormonal effects of pregnancy or increased pressure of carpal tunnel caused by child rearing.
Similar inconsistencies exist regarding the association between age at menopause and CTS. Although a study on 156 CTS cases and 473 controls could not show a clear relationship between age at menopause and CTS7 Kaplan et al.12 found significantly lower age at menopause in the postmenopausal women with CTS. In contrast, in the survey by Dieck and Kelsey14, postmenopausal women with CTS had a somewhat later age at natural menopause. The type of menopause, natural versus surgical, may affect the results of studies and explain some of disparities. Similar to our results, duration of menopause has not been shown to be different between postmenopausal women with and without CTS in a previous study.12
Toesca et al.4 evaluated the ER and PR expression in the specimens obtained from 30 CTS cases and four controls. Both TCL and synovial tissue from CTS patients expressed ERα, but PR was observed only in TCL samples and its appearance decreased with age. The number of ER- and PR-positive cells had no significant difference between men and women with the exception of the 50 to 70 year age group. Increase in the expression of ERα with age in women with a peak in menopausal age and then decrease in the elderly group can correlate with the nature of CTS disease affecting typically peri- and postmenopausal women. The number of ER- and PR-positive cells in non-CTS patients was significantly lower than that in CTS patients. Authors suggested that localization of the ER and PR proteins in the normal TCL is related to the theory that female sex hormones influence the physiological modulation of TCL metabolism.4 These receptors have already been supposed to have an effect on the structure of the ligaments in studies on human anterior cruciate ligament.15 Sex hormones fluctuations predispose this ligament to the higher injury rate in female athletes by changing their composition.1617 Toesca et al.4 supposed that fluctuation of estrogens and progesterone could similarly affect TCL through acting on fibroblast proliferation and collagen synthesis. Also, the effect of estrogen on synovial tissue was attributed to the immunomodulation of synovitis and synovial hyperplasia and the regulation of pro-inflammatory cytokines.4 We could not find such results in our study. The survey conducted by Toesca et al.4, had some limitations. It had a very small control size and did not exclude the patients with concomitant diseases like diabetes, rheumatoid arthritis, dysthyroidism (15 cases) and women treated with HRT. The possible effects of these confounding factors make the results of this study questionable.
Kim et al.3 evaluated ER expression in tenosynovial tissues of postmenopausal woman with idiopathic CTS and found enhanced expressions of ERα and ERβ in the tenosynovial tissues of them. Estrogens have anti-inflammatory properties, and menopause as a state of estrogen withdrawal is associated with elevated levels of inflammatory cytokines, such as interleukins and tumor necrosis factor-α (TNF-α).1819 It is proposed that upregulation of ERs in CTS patients compared to the controls implies that estrogen concentrations in tenosynovial tissue or systemically differ in CTS patients, however, systemic or local estrogen levels were not measured by Kim et al.3 at all and it was unclear that increased ER expression in postmenopausal women with CTS was prior to the onset of CTS or a secondary change. In the present study, we measured serum estrogen level and could not find any difference between CTS cases and controls. This finding undermines the theory proposed by Kim et al.3.
Kim et al.3 found no correlation between symptom duration or subjective symptom severity according to the Boston score and ERα and ERβ expression and concluded that expressions of ERs are not directly correlated with edematous swelling or angiogenesis of flexor tenosynovium. This conclusion was based on findings of a MRI study which showed that palmar bowing of the flexor retinaculum as a marker of tenosynovial edematous swelling correlate significantly with patients' subjective reports of pain severity.20 In the present study for concise evaluation of the relationship between CTS severity and sex hormone related factors, electrodiagnostic parameters as well as Boston score were measured for every patient. Similar to the study by Kim et al.3, no significant correlation was found between ER expression or serum estrogen level and Boston score. Also, no correlation was found between ER expressions or serum estrogen level and electrodiagnostic parameters.
The authors think that a significant difference in the hand and wrist anthropometric features in females with CTS, as compared to the females without CTS and men, can be the reason of inconsistencies in the results of different studies. Hand and wrist anthropometric features (higher wrist ratio, higher shape index, and narrower outlet) were found to be independent risk factors for CTS in females, but not in males.52122 Future studies should consider these factors as potential confounding factors while investigating the role of sex hormones in CTS.
There were some limitations in this study. The case sample size was small and we could not measure local estrogen levels; however, systemic estrogen level was measured for every case and control subjects. Also, we assessed only patients with severe CTS and this may be the cause for different results of our study compared to the previous surveys.
Finally, it should mentioned that sex hormones cannot still be considered as the etiology or the only predisposing factor of idiopathic CTS in postmenopausal women and the role of other factors such as wrist ratio and narrower outlet in females compared to the males should be taken into account while investigating the effect of hormonal issues on CTS.



 XML Download
XML Download