

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Mammography is an important diagnostic imaging modality for the early detection of breast cancer.1 Breast density is an important risk factor for breast cancer. Increased density is not only a risk factor for breast cancer, but it results in reducing the sensitivity and specificity of mammography.23 Breast density on mammography, is determined relatively with measured breast fat and fibroglandular tissue and also in dense breast tissue breast cancer risk is increasing 4 to 6 times more than in non-dense breast tissue. Mammographic density is determined qualitatively, quantitatively or by Wolfe classification or the Breast Imaging Reporting and Data System (BI-RADS) density score by using digital technologies.45
Breast density is influenced by many factors such as age and menopause. Breast density shows the geographic and ethnic differences.6 Also it is stated that postmenopausal hormonal therapy affect the sensivity and specificity of mammography.27 In addition, the patient's increased body mass index (BMI) reduces the density of mammography.8 Sung et al.9 reported that in premenopausal women there was a correlation between mammographic density and BMD, but in post-menopausal women this relation was not present.
Dense fibroglandular tissue can hide lesions or microcalcifications in mammograms and may reduce the sensitivity of mammography. Also increased mammographic density is a risk factor for the development of breast cancer.10 Therefore, in addition to the evaluation of the pathologies such as calcification, mass, etc. on mammography for breast cancer, the evaluation of the density is very important. Highlighted in this respect, effects of parameters such asage, duration and type of menopause, number of pregnancies, BMI, laboratory findings follicle stimulating hormone (FSH), luteinizing hormone (LH), estradiol (E2), thyroid stimulating hormone (TSH), hemogram sub parameters, liver enzymes, serum lipid levels (Triglycerides, Cholesterol, high-density lipoproteins [HDL], low-density lipoproteins [LDL]), bone density measurement on mammographic density were investigated in this study retrospectively.
Materials and Methods
1. Patient selection
Between January 2013 and January 2014, 215 patients admitted to the Clinics of Obstetrics and Gynecology with complaints of menopause were included in this study. Local ethics committee approval was obtained for the study (date / number: January 8, 2014 / 118). Data of the patients were obtained from hospital computer records and were analyzed retrospectively. The inclusion criteria are; (1) patients with last menstrual period one year before, (2) patients having surgical menopause, (3) achive the demographic and backround records of patients (age, thype of menopause, number of pregnancy, etc), (4) achive the laboratuary and mammographic records of patients, (5) no using any medication containing hormones. Included patients according to the mammography density were divided into two groups as group I (non dense, n = 175) and group II (dense, n = 40). BMI was calculated as the weight divided by the height squared (kg/m2).
2. Assesment of breast density on mammography
All images were obtained with Senoguard-750 mammography X-ray system. Mammographic breast density is recorded qualitatively in the Carolina mammography registry (CMR) using the American College of Radiology's BI-RADS classification, a standardized visual assessment metric that is routinely reported by same radiologists. BI-RADS density assessment defines four categories of breast composition including: (A) almost entirely fat, (B) scattered fibroglandular densities, (C) heterogeneously dense, and (D) extremely dense.11 Two groups were formed as groups A and B (non-dense), group C and D (dens). Breast density measured in the CMR is per woman and not per breast.
3. Statistical analysis
Statistics were run with software package STATA 11.0 (StataCorp, College Station, Texas, USA). Continuous variables were expressed as mean ± standard deviation (SD) or as median and categorical variables were expressed as percentage. The Chi-square test or Fisher's exact test was used, when appropriate to compare proportions. Continuous variables were compared by using an independent-groups Student's t-test if normality assumptions were met; otherwise, groups were compared using the Wilcoxon rank sum test. For the analysis of increased breast density, logistic regression was modelled. The model was constructed by backward selection of independent variables. Only variables with a P value < 0.05 were entered into the model. BMI, duration of menstrual interruption, number of pregnancies, parity, progesterone were defined as independent variables. A P value of < 0.05 was considered as statistically significant.
Results
1. Univariate analysis of demographic data
Analysis of demographic data of patients and statistical results were reported in details in Table 1. Thus; the patient's age, presence of concomitant disease (diabetes mellitus [DM], hypertension [HT], hyperlipidemia [HL], thyroid disease), previous surgeries (total abdominal hysterectomy [TAH] + bilateral salpingooophorectomy [BSO]), type of menopause (surgical or natural) and the patient's smoking habits were not risk factors for increasing density in mammography (P > 0.05). However; the low BMI, extension of the period of menstruation cut off, a few number of pregnancy found to be risk factors for increasing density in mammography (P < 0.05).
2. Univariate analysis of laboratory results
Between groups; the comparative results of gynecological hormones, complete blood count, biochemical parameters, serum lipid levels, thyroid function tests and bone density measurements are also seen in Table 2. There was no statistically significantly difference, in terms of FSH, LH, E2, TSH, hemogram sub parameters, liver enzymes, serum lipid levels (triglycerides, cholesterol, HDL, LDL), electrolyte levels and bone density in groups (P > 0.05). Progesterone levels were determined as significantly higher in the patients with dense breast group (P < 0.05).
3. Results of logistic regression analysis
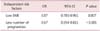
According to logistic regression analysis, the low BMI (odds ratio [OR]: 0.87, 95% confidence interval [CI]: 0.785-0.961, P = 0.007) and less number of pregnancies (OR: 0.67, 95% CI: 0.554-0.811, P < 0.001) were found to be independent risk factors for increasing densityin mammography (Table 3).
Discussion
Increased breast density on mammography is associated with breast cancer risk. The meta-analysis of 42 studies, the risk of breast cancer is 4.64 times greater in women with increased density than in women with low density has been found. The evaluation of breast density is relatively easy on mammography and can be used as an important parameter for early intervention and prevention of breast cancer.12 Therefore, knowledge of the risk factors that may lead to increased density in mammography and evaluation of patients with these risk factors will be important in the early detection of breast cancer. This study was performed to determine the risk factors of increased breast density and at univariate analysis the age, presence of concomitant disease (DM, HT, HL), type of menopause (surgery / spontaneous) and smoking habit have no relation with mammographic density, unlike our study, Martin et al.13 stated that breast density decreases with increasing age. However, in our study, chronological age was not an effective factoron breast density but breast density has increased in patients with longer duration of menopause. We believe that the difference between our study and the literature was there. In the literature, density reduced with age, but this change was not known inevery woman in uninterrupted (smoothor gradual) menopause, and the effect of the age on the breast density was not clearly defined.1415
Warwick et al.16 also showed that patient age was not an independent risk factor on breast density. Univariate analysis showed that the number of pregnancies and births, having a high BMI reduced breast density; the prolonged duration of menopause was found to be a risk factor that increase mammographic density. In this study, similar to previous studies, number of births and BMI in postmenopausal women were found to be risk factors affecting the mammographic density.812 Tsvetov et al.17 stated that there is inverse relation between the density and the number of births, and direct correlation between BMI and the density. Obesity increases the risk of breast cancer in postmenopausal women through a hormonal mechanism involving the metabolism of an androgenic precursor converted to estrogen in adipose tissue.67 While the obesity is a risk factor for increasing breast cancer, it seems to be a contradiction of breast density as being reverse correlated with BMI. But the fat in breast, epithelial and stromal breast tissue determine the mammographic density. Epithelial and stromal tissue are seen as dense on mammograms, adipose tissue is monitored as radiolucent. Therefore the adipose tissue takes place of breast tissue in obese women and is associated with an increase with non-dense area on the mammography.1518 In logistic regression analysis, pregnancy and BMI were identified as independent risk factors for breast density. BMI, pregnancy, menopause and age were found to be independent risk factors similar as in previous studies.16 Other studies also indicated an inverse relationbetween BMI and breast density.19 In our study smoking had no significant effect on breast density. Intake of alcohol affects the breast density, but it was confirmed that physical activity does not.512
In our study, there was no correlation between the breast density and serum lipid levels. Similarly, Tamburrini et al.20 stated that there was no relation between mammographic density and serum cholesterol diet in postmenopausal women. However Tehranifar et al.21 have shown the weak relation between high serum cholesterol levels and breast density.
Breast density is effected by ovarian steroid hormones. In maximum proliferation period of breast tissue, progesterone is at highest level. Progesterone increases breast epithelial proliferation and leads to increased breast density.2223 In our study, serum progesterone levels were significantly higher in women with increased mammographic density. Boyd et al.15 demonstrated that E2 levels are associated with mammographic density. However, in another study, total E2 and progesterone levels were unrelated with the mammographic density.14 In another article it was reported that there was no relation between ovarian hormone and breast density or there was a negative correlation.13
When we investigated the effects of postmenopausal hormone therapy on breast density, we observed that there was not a full consensus in the literature. For example Ellison-Loschmann et al.6 and Jackson et al.4 Reported that there was no effect on breast density as well as with 3-month and 12 months raloxifene therapy in postmenopausal women but they stated that the continuous combined hormonal therapy has increased the density. Kiran et al.24 reported that the 12-month 17β-E2 1 mg plus drospirenone 2 mg (E2 / DRSP) treatment increased the breast density. Colacurci et al.25 stated that 12 months combined regime therapy, especially progestin containing, effected the density but the type of treatment had no effect on density. Christodoulakos et al.26 stated that there was no change on the density with 12 months treatment in most patients. Junkermann et al.27 considered that the type of progesterone therapy had no effect on breast density.
In conclusion, in this study which examined the risk factors for mammographic density, in univariate analysis; higher BMI, the high number of births and pregnancy were found as risk factors that reduced breast density, while the high duration of menopause and high progesterone levels were found to be factors that caused an increase in breast density. In logistic regression analysis, the number of pregnancy and BMI were identified as independent risk factors for mammographic density. Accordingly, we believe that breast mammographic density measurement and the careful monitoring of individuals with risk factors for breast cancer would be important for the early diagnosis in breast cancer.


 XML Download
XML Download