

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Uterine lipoleiomyomas are rare benign neoplasms (incidence rate 0.03%-0.20%), and are recognized as a specific type of leiomyoma.1 These tumors are composed of an intimate admixture of smooth muscle cells and mature adipocytes.2 They are most commonly located in the uterine corpus, but rarely may be found in other locations, including the cervix, ovary, broad ligament, and retroperitoneum.234 Most patients are asymptomatic peri or postmenopausal women. Actually, uterine lipoleiomyomas are clinically similar to leiomyomas, and require no treatment if asymptomatic. Moreover, these tumors may be confused with other gynecologic conditions such as mature ovarian teratoma, well-differentiated liposarcoma, and atypical lipoma.23 Therefore, it is essential to distinguish these tumors from others that require surgical excision.2 We report six cases treated in our institution in order to contribute to the understanding of the characteristics of these tumors
Case Report
1. Case 1
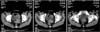
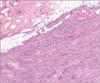
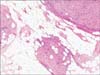
A 55-year-old perimenopausal, gravida 3, para 3 woman presented with gradual worsening of hot flashes, including night sweats for a few months prior to visiting her primary health care provider. Her abdomen was soft with no masses palpable. Transvaginal ultrasonography showed an echogenic 53 × 39 mm left adnexal mass. Tumor markers were within normal limits. Further evaluations were done in our gynecological outpatient clinic. Computed tomography (CT) was suspicious for a fatty pelvic mass of possible uterine origin (Fig. 1). Therefore, pelvic magnetic resonance imaging (MRI) was performed to determine whether the mass arose from the adnexa or the uterus. MRI revealed a fatty, heterogeneously enhancing mass in the subserosal layer of the anterior wall of the uterine body (Fig. 2). Total abdominal hysterectomy with bilateral salpingo-oophorectomy was performed, with a preoperative diagnosis of pelvis mass. Grossly, the uterus measured 8.6 × 5.5 cm and had two intramural and subserosal masses (4 × 3.5 cm and 2.4 × 1 cm), showing a whitish, whorling pattern of muscular bundles with firm consistency. Microscopically, the tumor tissue showed an admixture of smooth muscle and mature fat cells (Fig. 3). The highly cellular leiomyoma was composed of interlacing bundles of spindle-shaped smooth muscle cells, with no atypia or necrosis (hematoxylin & eosin [H & E] ×40; Fig. 4). The tumor contained mature fat cells (H & E ×100; Fig. 5). No other abnormal histopathological findings were noted and the diagnosis was confirmed as lipoleiomyoma. The patient is presently following-up regularly.
2. Case 2
A 45-year-old, gravida 1, para 1 woman was admitted to the gynecological outpatient clinic for premenstrual abdominal discomfort. She complained of abdominal bloating for 5 to 7 days preceding menstruation. The first day of her last menstrual period was seven days prior to the visit and the blood flow had been extremely light. Her medical and surgical history were significant in terms of cesarean section in 1997. A full-term-sized, slightly tender mass was palpated in the abdomen. On bimanual examination, the mass was solid, mobile, and pelvic in origin. Ultrasonography showed an approximately 20 × 18 cm, heterogeneous pelvic mass. Total abdominal hysterectomy was performed. Grossly, a 21 × 18 cm mass was separated from the left broad ligament, showing a relatively well-defined and whorling appearance on the cross section. Necrosis or hemorrhage was not present. The diagnosis of lipoleiomyoma-broad ligament was made.
Six cases of uterine lipoleiomyoma were identified from January 2005 to March 2015 in Dong-A University Hospital; 0.28% of patients with uterine leiomyomas during this period had a lipoleiomyoma (6/2129). The patients ranged in age from 45 to 70 years, with a mean age of 60.66 ± 9.20 years. The patients underwent a variety of surgical procedures. The majority of lipoleiomyomas were in the uterine corpus, but one was located in the broad ligament. In one case, we found a gynecologic malignancy and a stage 1A1 cervical cancer. Histologically, there was no gross or microscopic contiguity between the lipoleiomyoma and the malignancy. Two patients underwent exploratory laparotomies for a preoperative diagnosis of pelvic mass, and possible uterine sarcoma. Meanwhile, an exploratory laparotomy was performed for a preoperative diagnosis of right adnexal mass suggesting teratoma. Table 1 summarizes the cases of uterine lipoleiomyoma.
Discussion
Lipoleiomyomas are relatively uncommon fatty tumors of the uterus with an incidence rate varying from 0.03% to 0.20%.1 This tumor was first described as a myolipoma of the soft tissue by Meis and Enzinger5 in 1991.6 Uterine lipoleiomyomas are composed of benign smooth muscle cells with distributed and scattered lobules of adipose tissue, and may be concentrated in only focal areas, showing whorling of the lesions.7 There is no specific defined percentage of adipocytes that would enable a diagnosis of lipoleiomyoma.8 The majority of lipoleiomyomas are found in the subserosal or intramural uterine corpus, but some occur in the cervix, ovary, broad ligament, and retroperitoneum.234 Although rare, over 75% of retroperitoneal tumors are malignant.910 Actually, there is a report on surgery with a preoperative diagnosis mimicking retroperitoneal sarcoma in perimenopausal women; the diagnosis of uterine leiomyoma was confirmed.11 In our study, there was no retroperitoneal lipoleiomyoma. There was only one case wherein the lipoleiomyoma was located in the broad ligament; in all other cases, it was located in the uterine corpus.
The histogenesis of uterine lipoleiomyomas is uncertain. Immunohistochemical studies supported a complex histogenesis of lipoleiomyoma, which might arise from metaplasia of uterine smooth muscle cells, or from immature mesenchymal or ectopic embryonic fat cells.18 Nonetheless, fatty metaplasia is the most plausible theory, because there are no lipoblasts, atypia in adipocytes or smooth muscle cells, or necrosis.2
Uterine lipoleiomyomas generally occur in asymptomatic perimenopausal or menopausal women, while most leiomyomas tend to predominate in women of reproductive age. The clinical presentation of uterine lipoleiomyomas is similar to that of typical leiomyomas. Most patients are asymptomatic, although some present with menstrual abnormalities, abnormal uterine bleeding, a palpable mass, urinary frequency, or abdominal pelvic pain.12 If the patient complains of acute and persistent abdominal pain, the possibility of torsion needs to be considered. In reported case of torsion of subserosal leiomyoma, the patient was misdiagnosed as having secondary degeneration of uterine leiomyoma prior to the operation; she had suffered from abdominal pain for 2 weeks before surgery.13 However, in our cases, most symptoms were nonspecific, except for chronic pelvic pain. If asymptomatic, lipoleiomyomas require no treatment; it is therefore essential to distinguish these tumors from those requiring surgical excision.
Although the pathogenesis of uterine lipoleiomyomas is still ambiguous, it is known that some metabolic disorders, including hyperlipidemia, hypothyroidism, and diabetes mellitus are associated with lipoleiomyomas.1415 Changes in lipid metabolism related to estrogen deficiency after menopausal transition may play a role in their development.16 This hypothesis is consistent with the advanced age of our patients at the time of diagnosis. One recent study showed that hormone replacement therapy (HRT) did not change the size of uterine myoma significantly in menopausal women.17 However, studies on the effects of HRT on uterine lipoleiomyoma after menopause have not yet been reported. Therefore, further studies may be needed, considering the use of HRT in women with lipoleiomyomas.
The differential diagnosis of lipoleiomyoma includes benign cystic ovarian teratoma, ovarian lipoma, benign pelvic lipoma, liposarcoma, and carcinosarcoma.1 Uterine lipoleiomyomas are often diagnosed preoperatively as a uterine leiomyoma or a mature ovarian teratoma.6 Accordingly, we also performed pelvic MRI and abdominal and pelvic CT. Although imaging studies play an important role in preoperative localization and diagnosis of a lipoleiomyoma, pathological evaluation must be performed to confirm the diagnosis.1
Lipoleiomyomas seem to have a benign clinical course. However, lipoleiomyosarcomas arising in uterine lipoleiomyomas and intravenous lipoleiomyomatosis have been rarely reported.181920 Therefore, patients may be followed-up with routine gynecological examinations.8 Recurrence of some benign tumors after hysterectomy has been reported. For example, endometriosis occurred in a postmenopausal woman who underwent hysterectomy for uterine myoma 16 years prior.21 Until now, no recurrence of any benign tumors has been reported after hysterectomy for lipoleiomyomas. In our study, a mean follow-up period was 16.17 ± 23.80 months. There were no recurrences or deaths attributed to the lipoleiomyomas.
In conclusion, lipoleiomyomas are rare uterine tumors, and are considered a variant of uterine leiomyomas. Lipoleiomyomas are mostly seen in advanced age, and may be associated with estrogen deficiency after menopausal transition. Although lipoleiomyomas showed a favorable outcome in previous studies, regular follow-up may be needed in managing these patients.



 XML Download
XML Download