

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Ovarian hemangiomas are rare tumors and are usually found incidentally. In fact, fewer than 5 cases have been reported in the Korean literature and only around 50 cases in the English literature. Sizes of reported hemangiomas vary, and relatively few are large and symptomatic.
Histologic types of ovarian hemangioma include the cavernous and capillary types. However, most ovarian hemangiomas are of the cavernous type and consist of multiple, dilated, blood-filled vascular channels lined by a single layer of endothelium. Occasionally, ovarian hemangiomas are associated with hemangioma of the genital tract or other sites.1 Most patients experience relatively mild symptoms. Unusual manifestations associated with ovarian hemangiomas include thrombocytopenia,1 acute abdomen with ovarian torsion,2 calcification and resultant imaging misinterpretation,2 massive ascites and elevated cancer antigen (CA)-125 mimicking ovarian cancer,34 and hyperestrogenic or hyperandrogenic manifestations.5 Ovarian hemangiomas sometimes coexist with genital tract diseases or even malignancies,67 and thus, ovarian hemangioma can be clinically significant due to these occasional conditions.
Here, we report a case of ovarian cavernous hemangioma which manifested as a large growing mass in a postmenopausal woman, and present a brief review of the literature.
Case Report
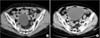
A 73-year-old woman with unremarkable medical and surgical histories presented with lower abdominal discomfort and cervical atypical squamous cells of undetermined significance (ASCUS). Physical examination revealed a palpable mass in the lower abdomen, and abdominopelvic computed tomography (CT) revealed a 12.1 × 9.0 cm sized, well-circumscribed mass, located anterior to the uterus, with thin septa attached to the right ovary (Fig. 1). The mass had been first detected 5 years previously when it was 6.4 cm sized. No ascites and no cutaneous or mucosal hemangioma were present. The patient was not receiving any hormonal medication, and her laboratory findings were normal; levels of the tumor markers CA-125 and CA 19-9 were within their normal ranges. At laparoscopy, the tumor was observed to be confined to the right ovary and to have a smooth purple colored surface. No evidence of torsion was noted, and the uterus, left ovary, and salpinges were unremarkable. The mass was totally resected. Its cut surface showed large cystic spaces, and intraoperative frozen section examination revealed it to be benign. The patient underwent bilateral salpingo-oophorectomy. Cytology results for peritoneal washings were negative for malignancy. Her postoperative recovery was uneventful, and she was discharged 4 days after surgery. Postoperative pathological findings revealed ovarian hemangioma of the cavernous type.
Grossly, the hemangioma weighed 19.1 g and measured 12.0 × 8.0 cm, and was multiloculated and contained blood clots (Fig. 2). Microscopically, it consisted of multiple, dilated, blood filled vascular channels separated by loose connective tissue (Fig. 3A), and all of these vessels were lined by a single layer of flattened endothelium (Fig. 3B). No mitotic activity was noted and no atypical cells were observed. Vascular spaces within the tumor varied in size. No heterotopic tissue elements were present, and the contralateral ovary and both tubes were unremarkable.
Discussion
Hemangioma of the ovary is rare despite the rich, complex ovarian vasculature.8 The majority are small, unilateral, and asymptomatic. However, large tumors present with symptoms, such as, swelling with ascites and abdominal pain, due to the mass per se or torsion. Ovarian hemangioma is mostly encountered incidentally at operation or autopsy. They may occur concomitantly with hemangiomas in the genital tract or other sites, and may cause abdominal and pelvic symptoms. Mass sizes range from 0.3 to 24 cm, and patient ages range from 4 months to 81 years, without no evidence of predominance in any age group.9
The etiology of ovarian hemangioma is controversial. Some have proposed that its pathogenesis may be stimulated by infection or hormones.3 They also constitute portions of mature teratomas or hamartomatous malformations.10 They would appear a failure of vascular formation, particularly of the canalizing process, results in the formation of abnormal vascular channels.8 Histologically, ovarian hemangiomas may be of the cavernous or capillary type, but the cavernous type is the most common. These types are differentiated by the sizes of blood vessels within tumors, that is, the capillary type consists of vessels of normal caliber, whereas the cavernous type contains larger vascular channels.
The most common locations of ovarian hemangioma are the medulla and hilar regions, which usually have larger vascular channels, and thus, ovarian hemangioma should be differentiated from proliferations of dilated blood vessels in ovarian hilum. These hemangiomas can be distinguished from hilar vascular proliferations when a circumscribed nodule or a mass is observed.11 Our case presented a well demarcated mass consisting of dilated vessels throughout the whole cystic lesion, which suggested ovarian hemangioma.
Clinical issues related to ovarian hemangioma are uncommon, but various, and include acute abdomen with ovarian torsion, calcification, massive ascites, co-occurrence with genital tract diseases, and hormonal manifestations (Table 1). Several cases of acute abdomen in patients with a twisted ovarian hemangioma sized from 6 to 18 cm,8 and several cases of calcified ovarian hemangioma have been reported.1213 Ovarian hemangioma should also be included in the differential diagnosis of adnexal masses with calcification. Unusual presentations including massive ascites and elevated CA-125 mimicking ovarian cancer have been reported.314 Kaneta et al.4 described a case of ovarian hemangioma with massive ascites, pleural effusion, and elevated serum CA-125 suggesting pseudo-Meigs' syndrome. The cause of the association between ovarian hemangioma and massive ascites has not been definitively identified, although vascular disturbance caused by hemangioma is a possible cause.15 Although highly unusual, ovarian hemangioma should be considered in the differential diagnosis of patients with ascites and elevated CA-125, for example, Akbulut et al.6 reported an ovarian hemangioma occurring synchronously with serous papillary carcinoma of the ovary.
In the majority of cases, ovarian hemangiomas are nonfunctional neoplasms, but functioning ovarian stroma containing luteinized stromal cells may result in hormonal effects. These cells produce androgen, which is subsequently converted to estrone in adipose tissue and finally causes unopposed estrogenic stimulation in endometrium. A few cases of ovarian hemangioma-induced endometrial stimulation have been reported. Endometrial hyperplasia or endometrial carcinoma associated with ovarian hemangiomas was reported.57 Shitsukawa et al.16 presented a case of ovarian hemangioma characterized by male pattern baldness and an elevated testosterone level.
Debate continues on the pathogenesis of ovarian hemangioma and its association with hormonal disorders. Carder et al.7 suggested preexisting stromal luteinization of ovaries might stimulate the development of ovarian hemangioma.
Imaging findings characteristic of cavernous ovarian hemangioma have been suggested. Yamawaki et al.15 described the CT and magnetic resonance imaging (MRI) findings of cavernous ovarian hemangioma. CT showed a complex mass with cystic and solid components, MRI showed a marked enhancement pattern on contrast-enhanced T1 weighted images. Although nonspecific, these findings are suggestive of ovarian hemangiomas. However, our case differs from previously reported cases, as CT did not visualize the pattern of characteristic hemangioma. It is possible MRI might help differentiate hemangioma and other tumors, but MRI was not performed in our case
In summary, we report a cavernous ovarian hemangioma that manifested as a large growing mass in a postmenopausal woman. Although the presence of ovarian hemangioma could not accurately predicted by preoperative CT, hemangioma should be considered in the differential diagnosis when a growing adnexal mass or a hemorrhagic ovarian lesion (Fig. 2) is encountered in postmenopausal women.



 XML Download
XML Download