

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Endometriosis is a benign disease involving ectopic endometrial glands or stroma that abnormally adhere to and spread to tissue outside of the uterus.1 Endometriosis is an estrogen-dependent disease that usually occurs in women of reproductive age. Postmenopausal endometriosis is rare, because the absence of estrogenic hormone production should prevent estrogen-dependent endometriosis.2 The incidence of endometriosis in postmenopausal women is low and estimated to be 2-4%.3 It has been suggested that hormone replacement therapy (HRT) can reactivate residual endometriosis or even produce new implants in climacteric women with a history of endometriosis.4 We report a case of endometriosis presenting in a postmenopausal woman with no history of endometriosis before menopause and review the literature.
Case Report
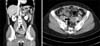
A 51-year-old woman, weighing 53 kg and 150 cm tall, presented with abdominal pain. The multiparous woman had undergone menopause at 45 years of age. Subsequently, she took HRT for 5 years and was in good general health until an ovarian tumor was detected on ultrasonography. She had no family or personal history of endometriosis. A pelvic ultrasound revealed a 2.5 × 2.5 cm left ovarian homogeneous cystic mass (Fig. 1). Computed tomography (CT) revealed a high-density 3.8 cm left adnexal cystic lesion (Fig. 2). Her cancer antigen (CA) 125 level was 551.9 U/mL (normal < 35.0 U/mL). The other CA serum markers (alpha-fetoprotein, carcinoembryonic antigen, CA 19-9, and beta human chorionic gonadotropin) were within their normal ranges. The data and image suggested a provisional diagnosis of left ovarian endometrioma. She was followed in our outpatient department for 6 months and the cystic tumor grew larger. However, the CA 125 level decreased to 62.1 U/mL. She decided to undergo a laparoscopic left salpingo-oophorectomy, which revealed a cystic left adnexal mass. Chocolate-colored fluid was observed in the ruptured ovarian cyst. Pathological examination of the excised tumor confirmed that it was an ovarian endometriotic cyst.
Discussion
Postmenopausal endometriosis is a rare disease, which was first reported in 1950. Endometriosis was found in 22% of 903 postmenopausal women.5 Regardless of the origins of the lesions themselves, endometriosis is widely considered to be an estrogen-dependent disorder.6 In postmenopausal women, estrogen is produced mainly in the skin and adipose tissue.6 Obese postmenopausal women produced much more endogenous estrogen than non-obese women, which may result in elevated serum estradiol levels.6 The use of HRT can cause an increased, although undefined, risk of recurrent endometriosis, especially in obese patients.7 HRT might cause endometriosis-associated symptoms in the postmenopausal population.7 Our patient had no history of gynecologic problems and developed endometriosis after menopause while on HRT.
Although postmenopausal endometriosis is usually benign, it is important to be aware of this condition, as it is increasingly recognized to have malignant potential.8 The reported frequency of malignancy transformation is 0.7-1.0%.9 After removing an endometriotic cyst, we should follow the patient because of possible malignant transformation.
We experienced a case of postmenopausal endometriosis during HRT. Endocrinologists prescribing hormone replacement therapy should be aware of this condition.

 XML Download
XML Download