

 PDF
PDF ePub
ePub Citation
Citation Print
Print


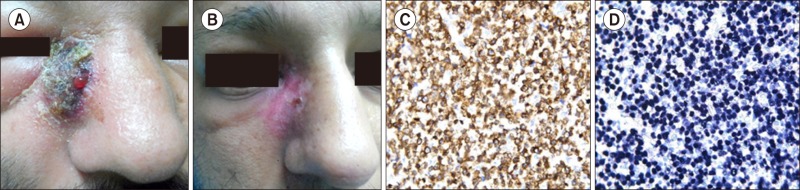
A 30-year-old man of Indian origin complained of a two-month-old ulcer on his face that remained unhealed. He denied any nasal obstruction, epistaxis, headache, or fever. A painless crusted lesion (5×5 cm) with surrounding induration localized over the right side of the nose along with periorbital edema (A) was observed. There was no pallor, palatal lesion, nasal mass, lymphadenopathy, or hepato-splenomegaly. A punch biopsy from the edge of the lesion was suggestive of extranodal natural killer (NK)/T-cell non-Hodgkin's lymphoma (NK/T-NHL), nasal type. Immunohistochemistry revealed positivity for cytoplasmic cluster of differentiation (CD) 3 and 56, granzyme B, and Epstein-Barr virus (EBV)-encoded-RNA by in-situ hybridization (EBER-ISH) thereby confirming the diagnosis of NK/T-NHL, nasal type (C, D). Peripheral blood analysis by polymerase chain reaction revealed 1,200 copies/mL of EBV-DNA. PET-CT scan, and MRI of orbit localized the disease to skin and subcutaneous tissue of the face (extranasal), with no periorbital extension. Blood investigations revealed a normal complete blood count (CBC), renal and liver function tests, and normal lactate levels. Treatment with chemotherapy (SMILE protocol: Steroids, Methotrexate, Ifosphamide, L-asparaginase, and Etoposide) and sandwiched radiotherapy led to complete resolution of the disease, as assessed by a repeat PET-CT scan (B). Extranodal NK/T cell lymphomas, nasal type, are highly aggressive neoplasms of the upper aerodigestive tract, constituting about 5–15% of NHL in Asian countries. ‘Isolated’ cutaneous involvement in NK/T NHL, nasal type, is rare, mandating its awareness amongst hematologists.
 XML Download
XML Download